Summary
This Briefing outlines the findings of the first analysis of national-level epidemiological trends in sepsis in Aotearoa New Zealand (NZ). We observed a 78% increase in sepsis-associated hospitalisations (SAH) between 2000 and 2019, with the highest rates for those <1 year or ≥70 years, Māori and Pacific peoples, and those living in areas of high socioeconomic deprivation. Most patients survived to discharge, and risk of death decreased by 50% over this study period. However, in-hospital deaths from a SAH represented almost 5% of total mortality in NZ between 2000 and 2019, with significant disparities between patient populations.
Our findings highlight an urgent need for a coordinated national plan to address the large, increasing and inequitable burden of sepsis in NZ. We propose a multifaceted approach for sepsis prevention and long-term harm reduction by focusing on Te Tiriti-aligned and Māori and Pacific co-designed strategies, infection prevention, antibiotic stewardship, early recognition, rapid treatment, post-sepsis care and rehabilitation, improved data collection and surveillance, as well as improved health literacy.
Historically referred to as blood poisoning or septicaemia, sepsis is a life-threatening condition arising when the body's response to infection injures its own tissues and organs.1 Globally estimated to cause one in three deaths annually,2 sepsis is the main biological pathway through which acute infection and diverse infectious organisms lead to severe illness and death. It is expensive to treat and leaves many survivors with serious ongoing disabilities.
Sepsis risk is highest for < 1 year and ≥70 years and those experiencing economic or ethnic marginalisation. In NZ, sepsis-associated hospitalisations (SAH) show marked disparities in incidence with poor outcomes for Māori and Pacific peoples, and those living in areas of high socioeconomic deprivation.3-5 With an ageing population, the increasing prevalence of predisposing factors such as diabetes, obesity and multimorbidity, sepsis incidence in NZ is likely increasing.
This Briefing outlines the findings of our new research, published in Lancet Regional Health: Western Pacific, which reports the burden of sepsis in NZ by estimating national-level trends in SAH incidence and mortality rates, and case fatality risk between 2000 and 2019, by major sociodemographic characteristics.6
Incidence and mortality from sepsis and temporal trends
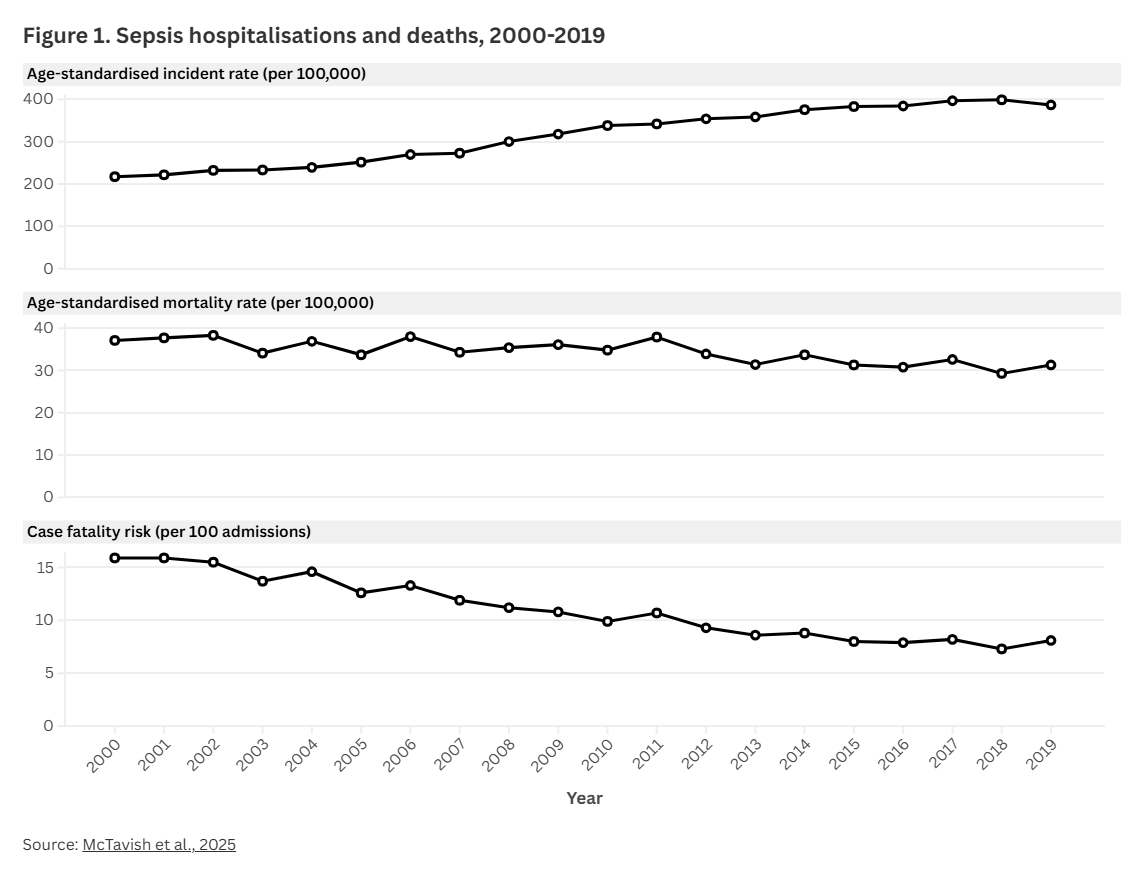
Between 2000 and 2019, we identified 266,105 unique SAH, an average of 13,305 per annum, with an average age-standardised sepsis-associated hospitalisation (ASAH) rate of 320.4 admissions per 100,000 population. There were 27,402 associated in-hospital deaths, which represented 4.5% of the total 609,000 deaths over that period, an average of 1,370 per annum, and an age-standardised sepsis mortality rate (ASMR) of 34.2 deaths per 100,000 population (Figure 1).
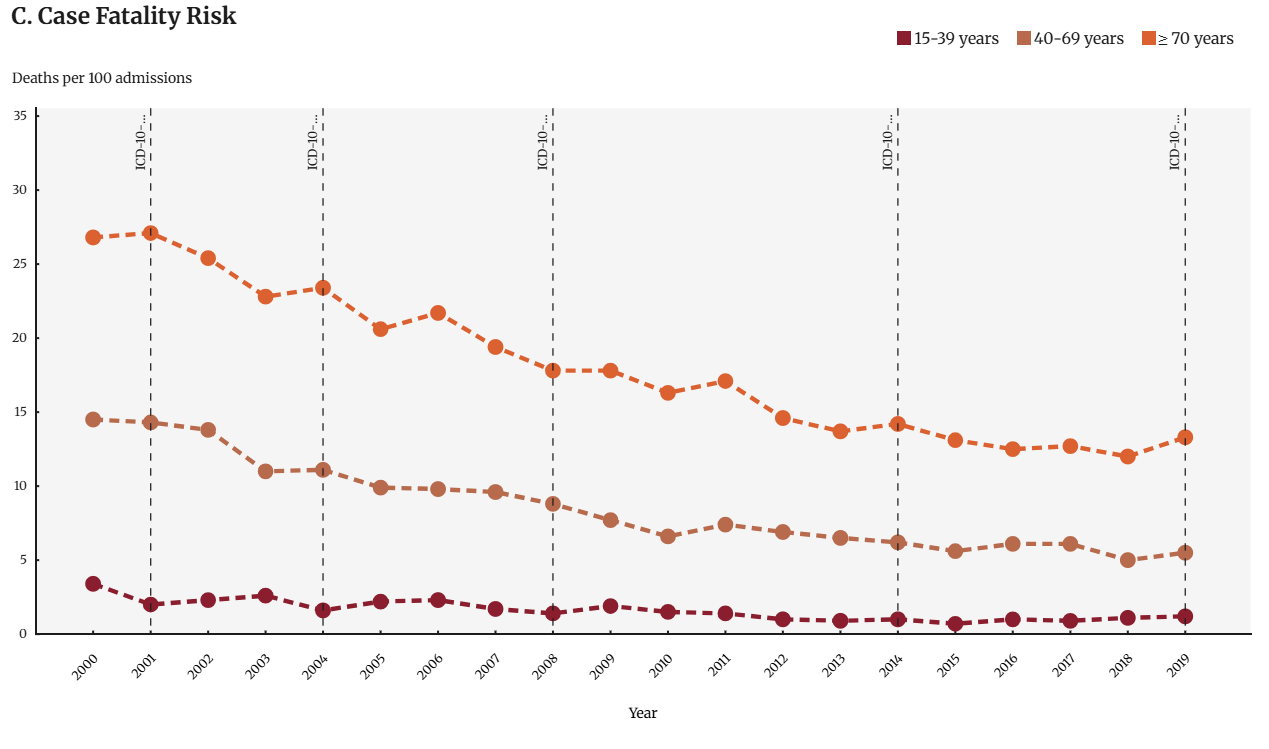
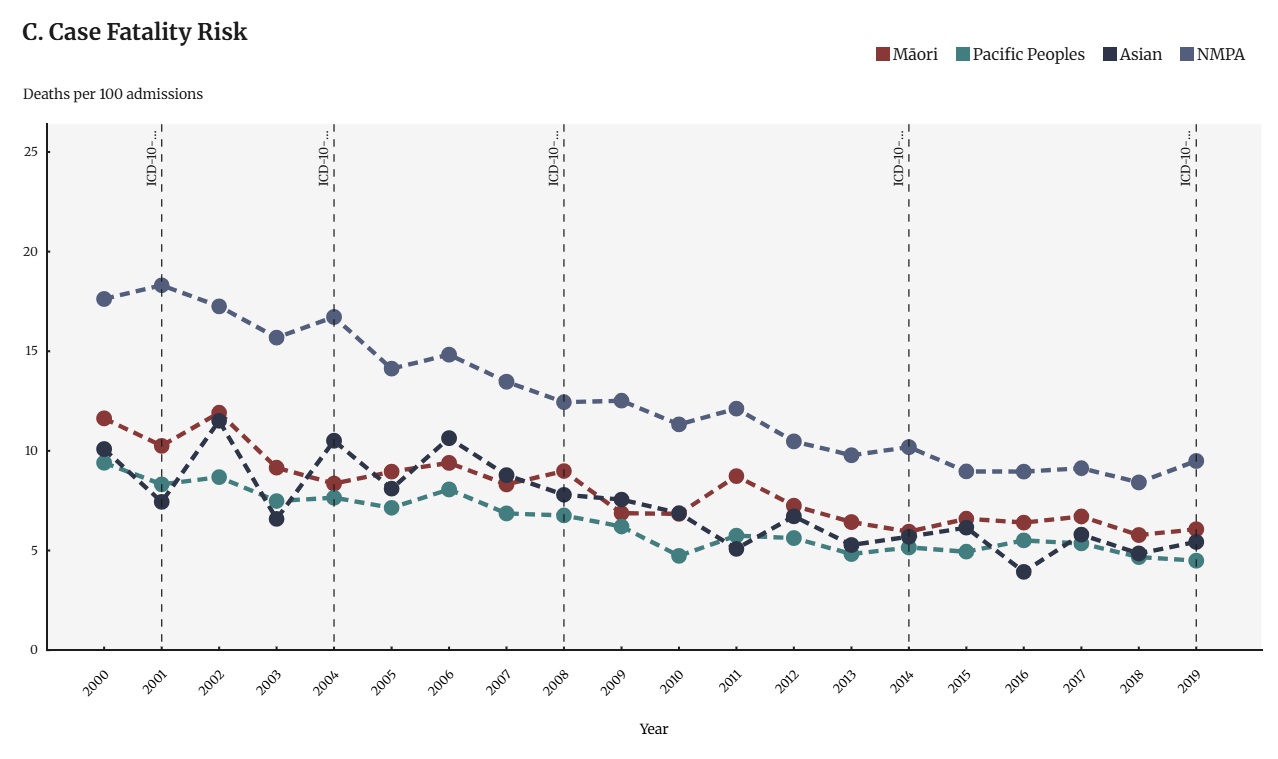
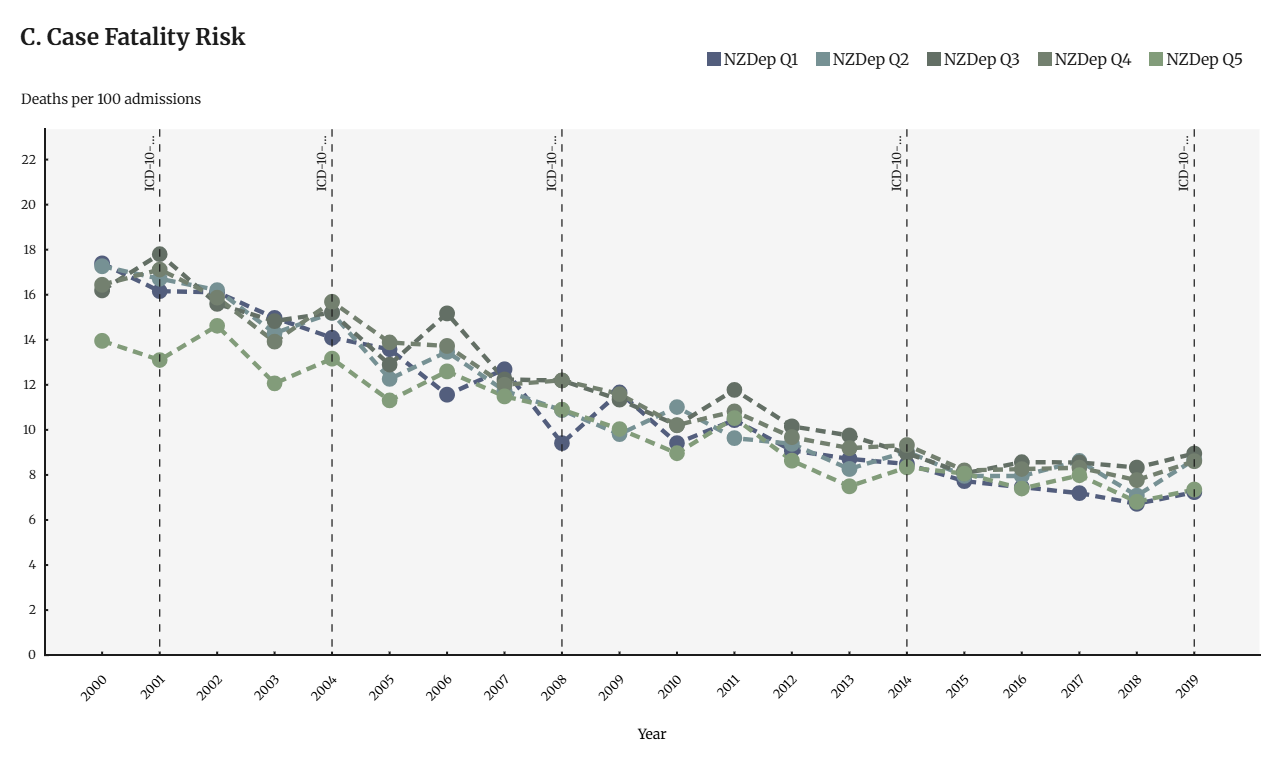
ASAH incidence increased from 217.3 admissions in 2000 to 386.9 admissions per 100,000 population in 2019, a 78.0% increase. ASMR decreased from 37.1 deaths in 2000 to 31.3 deaths per 100,000 population in 2019, a 15.6% decrease. Case fatality risk decreased substantially from 15.9% in 2000 to 8.1% in 2019, primarily driven by improvements in patient survival in ≥ 40-year age groups.
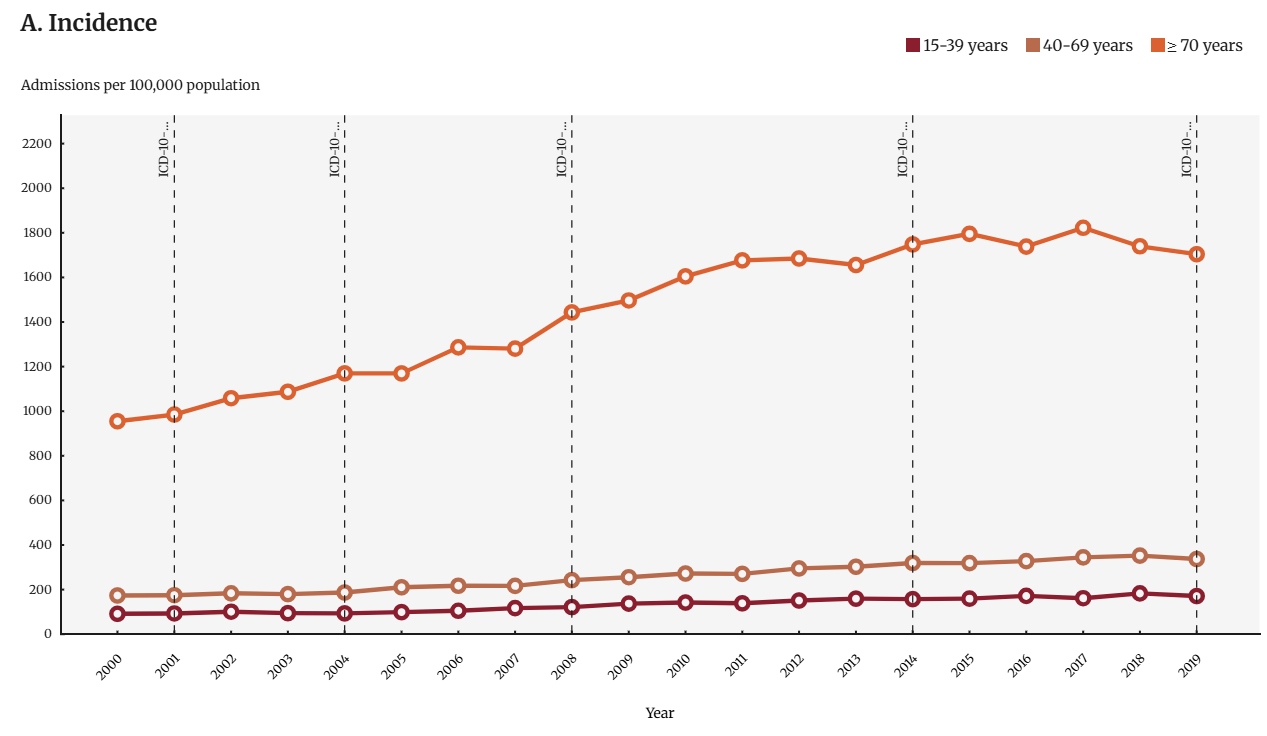
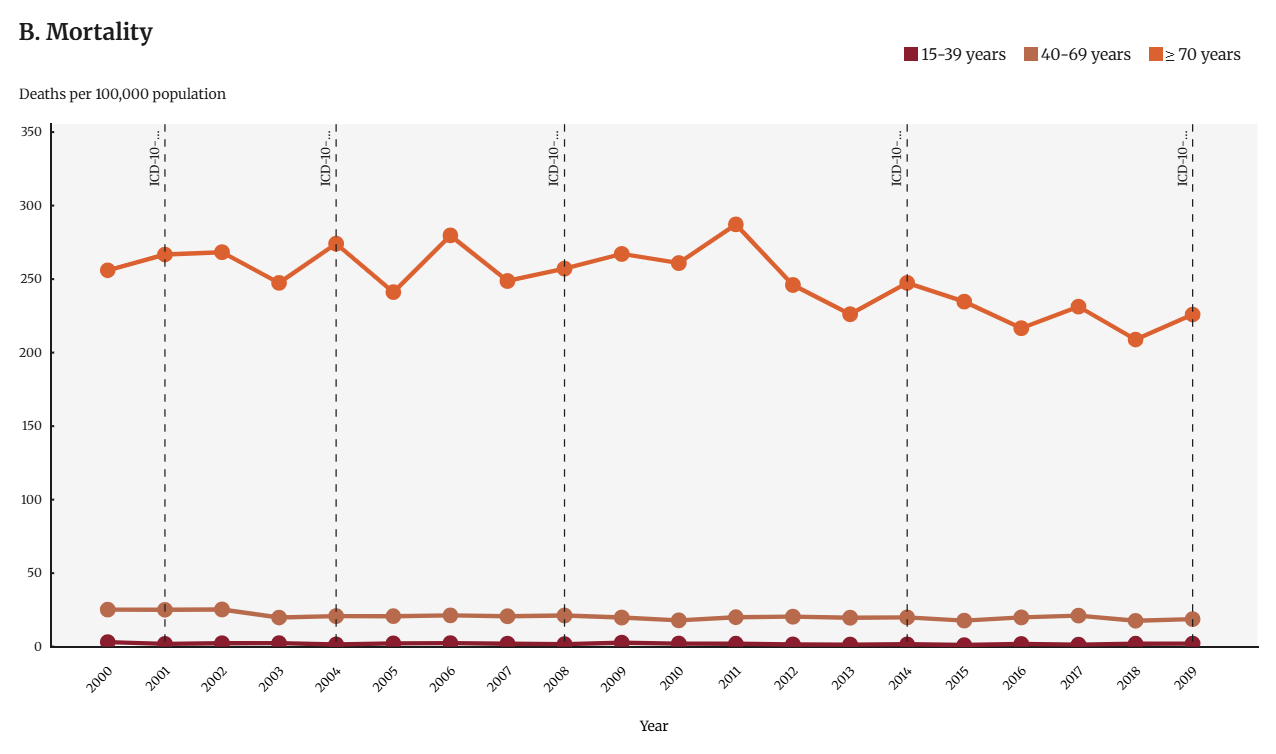
Sepsis incidence and hospitalisation outcomes were strongly influenced by age. We consistently observed the highest incidence and mortality rates, and case-fatality risk in patient populations aged <1 year and ≥70 years. The increase in incidence was particularly marked among patients aged ≥ 40 years (Appendix, Figure A1). In contrast, incidence among paediatric patients remained relatively constant.
Disparities by ethnicity and socioeconomic deprivation
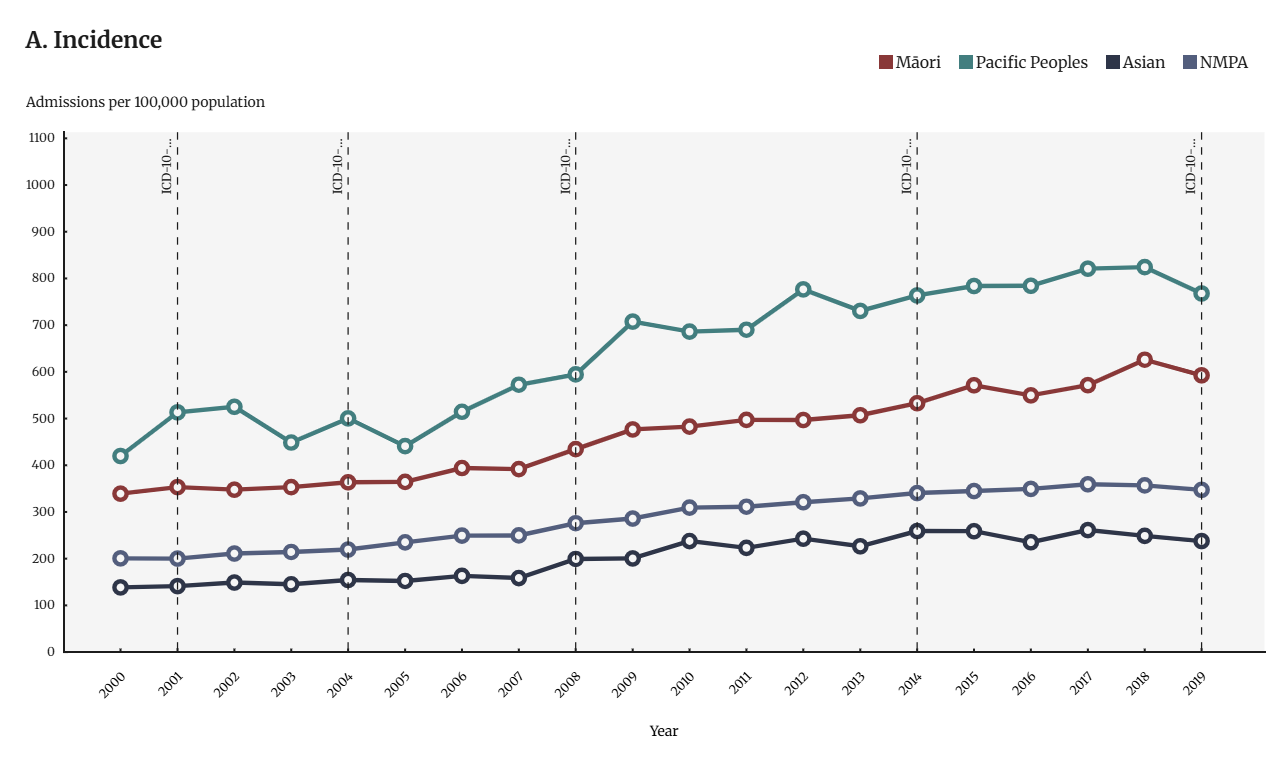
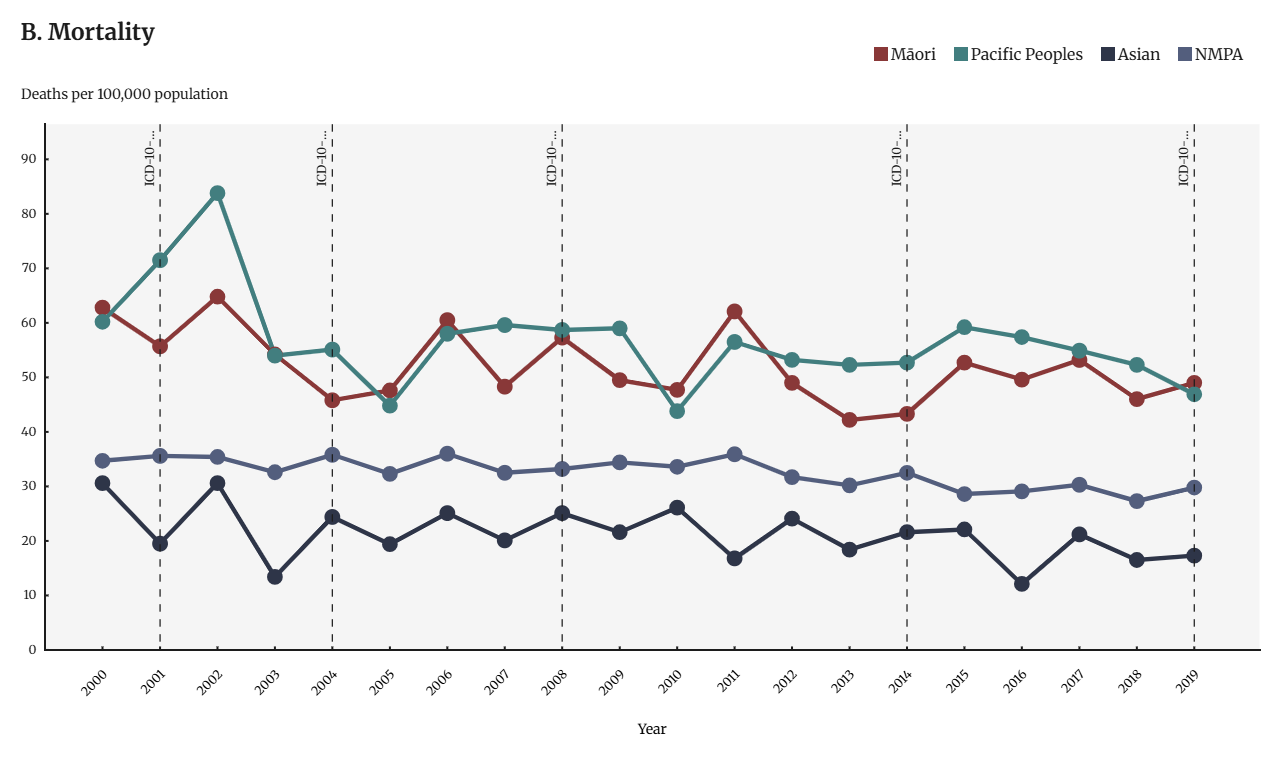
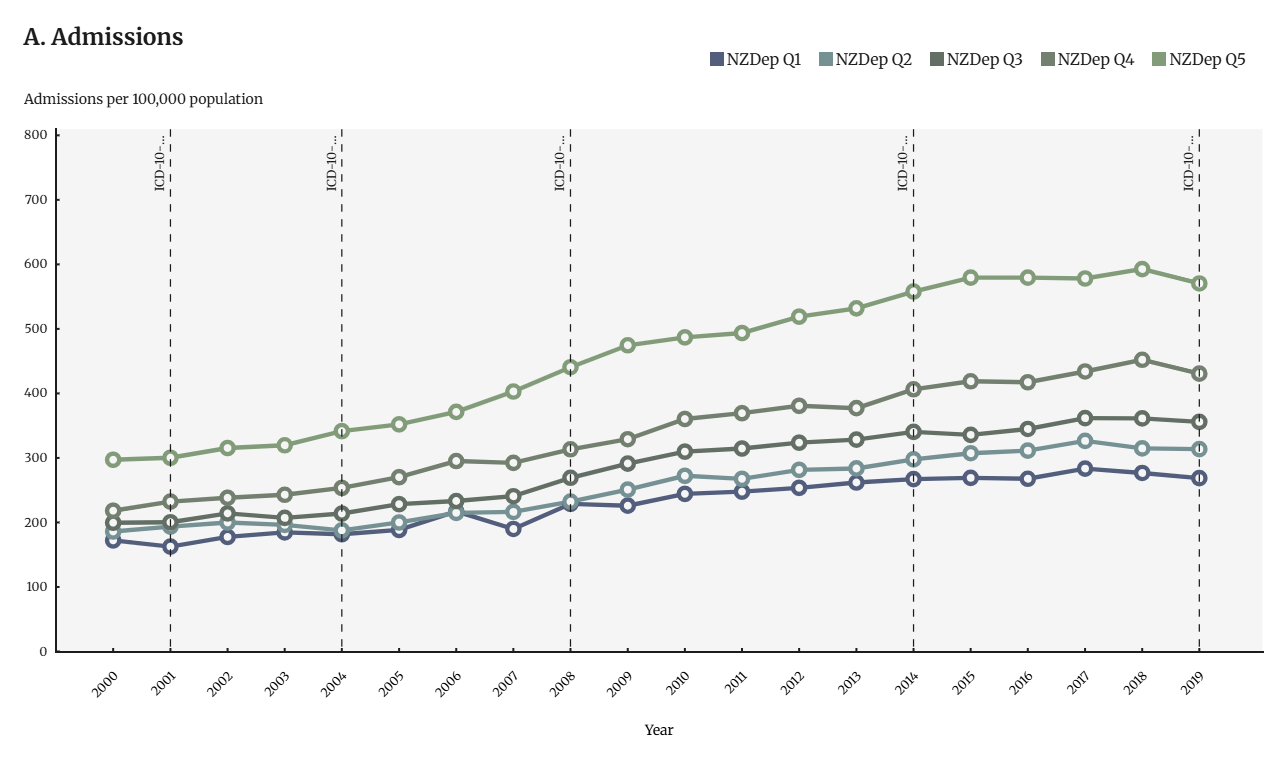
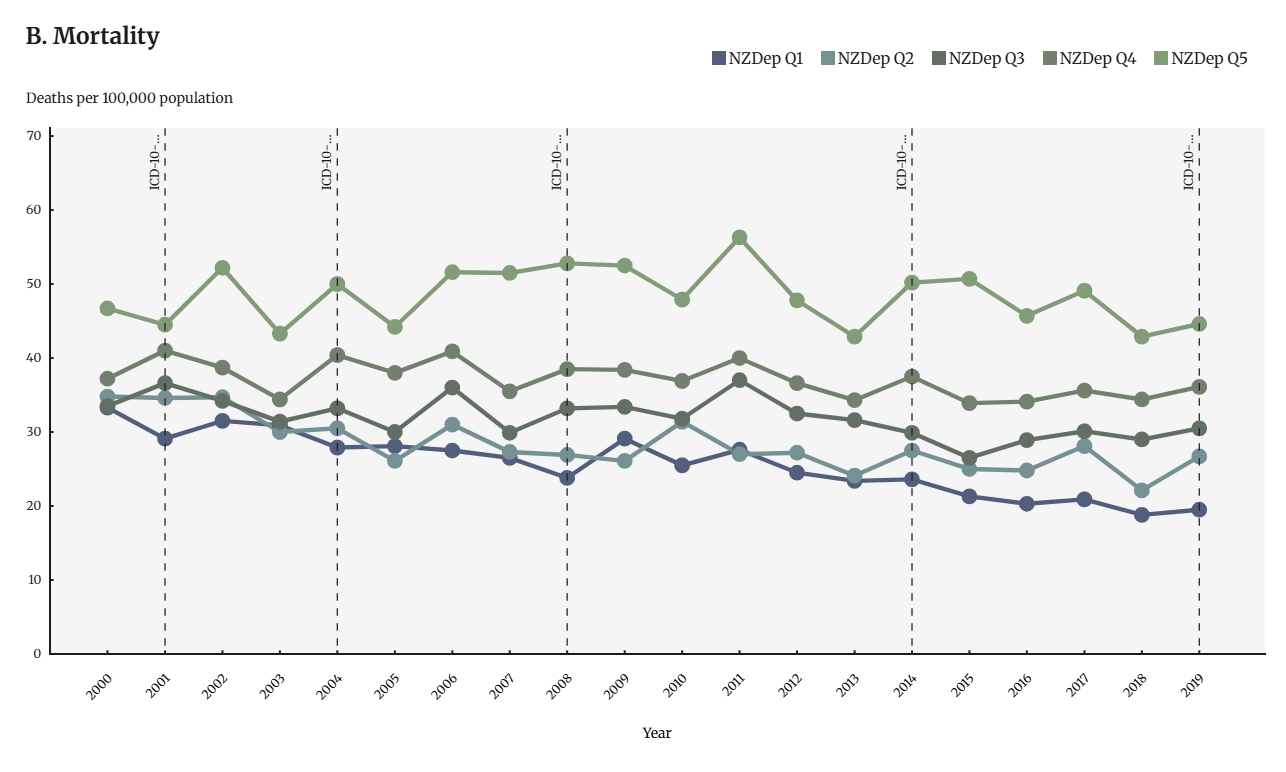
Significant and sustained SAH incidence and mortality disparities were observed between patient populations by ethnicity and socioeconomic deprivation, particularly for Māori and Pacific Peoples (Appendix, Figure A2), and those living in areas of high socioeconomic deprivation (Appendix Figure A3). Māori and Pacific Peoples were 66.0% and 131.0% more likely to develop sepsis and were 59.0% and 77.0% more likely to die during a SAH, respectively, than Non-Māori/Pacific/Asian (NMPA) peoples. Comparatively, Asian peoples were 31.0% less likely to develop sepsis and 38.0% less likely to die during a SAH than NMPA peoples. People living in areas of high socioeconomic deprivation (NZDep Q5) were 97.0% more likely to develop sepsis and 95.0% more likely to die during a SAH compared to people living in areas of the least deprivation (NZDep Q1).
Responding to the high and inequitable rates of sepsis
Given the large, increasing, and inequitable burden of disease from sepsis, we consider there is a strong need for the government to develop and implement a national sepsis action plan. This action would align with research evidence 2-8 and would support commitments made by NZ as a member of the World Health Assembly, and the work of the Accident Compensation Corporation, the Health Quality and Safety Commission, and national advocacy groups, including the Royal Colleges and the Sepsis Trust NZ. 9-15
We consider that such a plan should include the following elements:
- National leadership and coordination – Establish a governance and steering group to oversee the development and implementation of a nationally coordinated sepsis action plan with clear targets, accountability, and consistent reporting.
- Equity-focused approach – Embed Te Tiriti–aligned, Māori and Pacific co-designed strategies to reduce inequities in incidence and outcomes.
- Infection prevention – Strengthen access to vaccination, chronic disease management, primary care, improved hospital infection control and targeted antimicrobial stewardship.
- Early recognition and rapid treatment – Standardised screening tools, rapid treatment protocols including high-risk stratification strategies, workforce education, electronic alerts to reduce delays to antibiotic delivery and promotion of sepsis recognition as a key component of antimicrobial stewardship.
- Post-sepsis care and rehabilitation – Structured follow-up with equitable access to therapeutic and rehabilitation services, and GP awareness of post-sepsis complications.
- Improved surveillance and research – Standardised sepsis coding, real-time monitoring, linked datasets, public engagement in reporting of outcomes and targeted research funding.
- Public awareness and health literacy – Culturally appropriate, community co-designed campaigns to promote early recognition of infection, sepsis and timely care-seeking.
What this Briefing adds
- Reports on the results of the first comprehensive analysis of epidemiological trends in the incidence and outcomes of sepsis in Aotearoa, based on age-standardised incidence and mortality rates, and case fatality risk over 20 years (2000-2019).
- Findings indicate sepsis is increasingly common in Aotearoa, with a 78.0% incidence rate increase between 2000 and 2019, and an average of 13,305 SAH per annum.
- Sepsis is a major cause of mortality, with an average of 1,370 deaths in hospital per annum, which represented 4.5% of total deaths, though the ASMR has declined over that period.
- Sepsis incidence and mortality are strongly influenced by the social determinants of health, with markedly elevated rates for Māori, Pacific people and those living in more deprived neighbourhoods.
Implications for policy and practice
- Sepsis deserves considerable attention based on its high and increasing incidence, large contribution to mortality, increasing numbers of survivors with ongoing support needs often borne by whānau and communities for years, and stark disparities between patient populations.
- We recommend a comprehensive sepsis action plan codesigned by all relevant agencies and community representatives to address prevention, early treatment, long-term recovery and equity, supported with effective leadership, surveillance, research and public awareness.
Authors details
Sharla McTavish, Tangata Tiriti PhD student, Department of Public Health, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington
Jane Zhang, Research Fellow, Department of Public Health, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington
June Atkinson, Senior Analyst, Department of Public Health, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington
Assoc Prof Amanda Kvalsvig, Department of Public Health, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington
Alice Hyun Min Kim, Senior Research Fellow / Biostatistician, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington
Dr Colin McArthur, Auckland Hospital | Te Toka Tumai Auckland, University of Auckland | Waipapa Taumata Rau
Dr Paul Huggan, Waiora Waikato Hospital | Te Whatu Ora Waikato, University of Auckland | Waipapa Taumata Rau, Sepsis Trust NZ
Prof Michael Baker, Department of Public Health, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington, and Director, Public Health Communication Centre
Appendix
Figure A1: Adult (≥15 years) SAH incidence (A) and mortality rates (B), and case-fatality risk (C) in Aotearoa, between 2000 and 2019, by age bracket. Time points where the ICD-10-AM coding changes occurred in the National Minimum Dataset are also identified.
Figure A2: Adult (≥15 years) SAH incidence (A) and mortality rates (B), and case-fatality risk (C) in Aotearoa, between 2000 and 2019, by ethnicity. Time points where the ICD-10-AM coding changes occurred in the National Minimum Dataset are also identified. NMPA: (Non-Māori/Non-Pacific/Non-Asian)
Figure A3: Adult (≥15 years) SAH incidence (A) and mortality rates (B), and case-fatality risk (C) in Aotearoa, between 2000 and 2019, by socioeconomic deprivation. Time points where the ICD-10-AM coding changes occurred in the National Minimum Dataset are also identified. Values presented by NZDep quintile, from areas of the least socioeconomic deprivation, NZDep Q1, to areas of the highest socioeconomic deprivation, NZDep Q5.