In this blog we consider the ‘Auckland August cluster’ in the light of the changing landscape of international evidence about COVID-19 risk for children and young people. The high proportion of Pasifika children and young people in the Auckland outbreak may be a preview of what an uncontrolled COVID-19 pandemic would look like in Aotearoa New Zealand. There is an urgent need to improve coordination of child-centred policy in the COVID-19 response with better Māori and Pasifika representation in decision-making at all levels. Immediate actions include mandating mask use for secondary-age children at Alert Levels 2 and 3 and encouraging primary-age children to make and use masks.
The SARS-CoV-2 virus is a new pathogen, requiring pandemic response strategies to be built on evidence that has uncertain aspects and is evolving. Globally, we are now seeing the beginning of what may be a major shift in the assessment of COVID-19 risk for children and young people (CYP). For example, the World Health Organization (WHO) has now recommended mask use in children 12 years and over,1 to bring them into line with recommendations for adults.
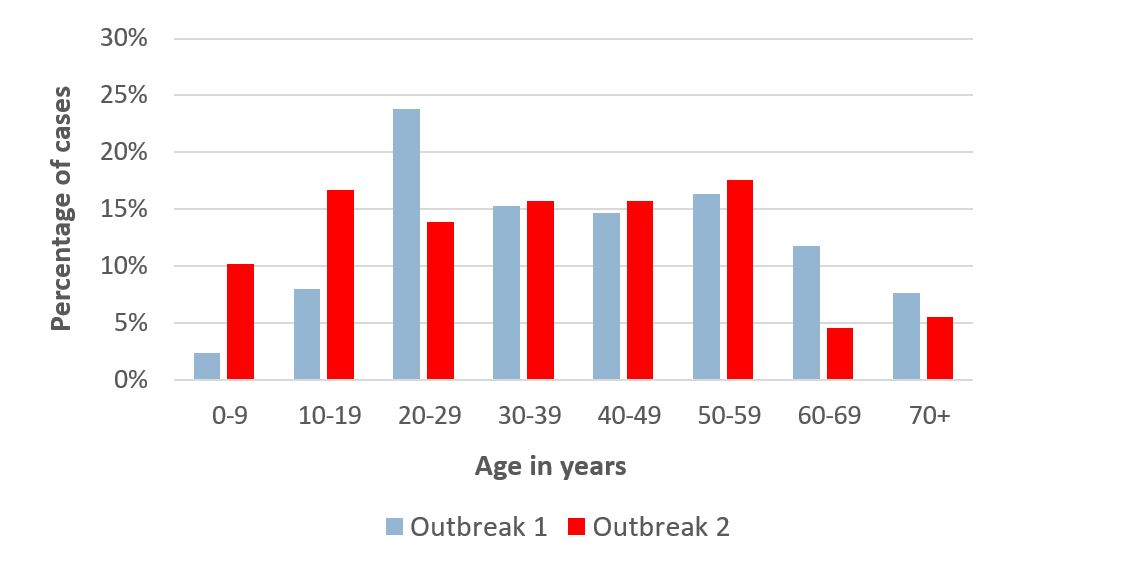
This evidence is emerging at a time when we have seen an unexpectedly large number of cases in young age-groups during NZ’s second outbreak (Figure 1). At the time of writing (26 August 2020), just over a quarter (29/108) of the cases in Outbreak 2 have been under 20 years (10% aged 0 to 9 years, and 17% aged 10 to 19 years), and 74% of the cases identify as Pasifika.
Figure 1. Differences in age distribution of COVID-19 cases between New Zealand’s Outbreak 1 (February to May; 1506 cases) and Outbreak 2 (August; 108 cases). Data from the NZ Ministry of Health.
Changing evidence about COVID-19 risks for (and from) children and young people
Early reports suggested that COVID-19 was typically a mild and self-limiting disease in children, with a very low risk of death or severe complications,2 and low risk of child-to-child and child-to-adult transmission.3 This perception of low risk has shaped a number of decisions around pandemic response measures, but it is being challenged by new research.
Evidence gaps about CYP have included the following:
- The true incidence of childhood COVID-19 has probably been underestimated because children frequently have a mild or asymptomatic clinical course. Children have not been prioritised for testing,4 5 especially where testing resources are constrained. They have been reported to excrete virus at similar levels to older age-groups,6 and the implications of this finding for onward transmission remain unclear.
- Earlier outbreak investigations did not identify schools as important settings for transmission but schools have largely been closed during lockdowns and for Northern Hemisphere summer holidays. Numerous school-based outbreaks are being reported as schools and universities reopen, and young adults now contribute a high proportion of cases worldwide.7
- Post-infectious complications take time to emerge and were not initially understood to be a significant feature of COVID-19 infection. It is now clear that post-infectious phenomena such as fatigue are common even with a history of a mild acute infection. Several case series are reporting uncommon but serious and life-altering complications in CYP, including Paediatric Inflammatory Multisystemic Syndrome (PIMS)8 and Type 1 diabetes.9
- Infectious disease outbreaks are always shaped by context. Because NZ rapidly eliminated COVID-19 initially, we have very little direct experience of how the pandemic interacts with structural conditions in NZ. These conditions include unaffordable housing driving household crowding, structural racism leading to unequal access to healthcare, and high prevalence of child obesity.10 11 Māori and Pasifika have experienced devastating losses in previous pandemics and the above risk factors strongly suggest that a future uncontrolled COVID-19 outbreak would be patterned in similar ways. (See the Appendix ‘Reasons to be concerned about COVID-19 in Aotearoa NZ if elimination fails’ for more detail).
What the NZ Government needs to do now
International and local experience demonstrates the danger of assuming that CYP are generally unaffected by COVID-19 and play no significant role in its transmission. The high proportion of Pasifika children in the Auckland outbreak is a particular concern.
To ensure successful elimination of future community outbreaks and protect CYP and their families, changes to current policy and practice are now indicated.
- Children and young people should use face masks, as advised by the World Health Organization (WHO), to prevent transmission in school-related and public settings. In NZ, measures should include:
- Introduction of mandated mask use in secondary schools and school buses at Alert Levels 2 and 3 (and also if variants such as 2.5 are created). More generally, mask use in adolescents should be brought into line with recommendations and mandates for mask use by adults;
- Activities to promote making and wearing masks in primary schools (at present the WHO does not recommend masks for children under 5 years). The evidence for transmission in primary-age children remains unclear currently, but uptake by children can help to normalise mask-wearing in communities (as happens with other health-promotion messaging such as handwashing and sun protection), and these activities will allow mask use to be up-scaled quickly if new evidence supports its value in primary-age children;
- Any measures to recommend or require mask use should also include provisions for CYP who are unable to wear a mask, and CYP who rely on seeing faces to access communication (eg, by providing masks with clear panels).
- There needs to be a comprehensive review of measures to protect school-age CYP in NZ from the impacts of both the pandemic and the response, balancing the risks and benefits of onsite teaching during a community outbreak. Considerations include:
- The feasibility and effectiveness of a suite of control measures to reduce close contact and viral transmissibility during the school day (including masks, cohorting, use of CovidCards to track contact patterns, outdoor learning, restriction of indoor sports, dance, and choir activities);
- Systems and support to ensure that if offsite schooling is indicated, the education of children from low-income families is not additionally compromised (eg, rapid provision of devices, internet, resource packs, tutoring and mentoring);
- Systems and support to ensure that if offsite schooling is indicated, the non-education-related wellbeing of CYP is not additionally compromised (eg, re-orientating provision of counselling, meals, child protection, and other support provided in school settings).
- The wellbeing of children and young people must be protected in all aspects of pandemic planning and response. The Government has a duty to align its COVID-19 response to the principles of the UN Convention on the Rights of the Child. To ensure compliance, a COVID-19 child wellbeing lead should be appointed as part of the All-of-Government response, and each agency involved in the response should have a designated children’s lead. Child-centred actions could include support for working parents to remain at home with an unwell child; age-, culturally-, and language-appropriate information for CYP about the pandemic and response measures, active monitoring of CYP wellbeing both on an individual and population basis, and amplifying the voices of CYP as they identify problems and solutions relating to the COVID-19 pandemic and response. Māori and Pasifika should be key decision-makers at all levels of the response.
Concluding comments
NZ successfully eliminated its initial COVID-19 outbreak and is likely to be able to eliminate the second outbreak (the current ‘Auckland cluster’). The country’s long history of infectious disease inequalities, and the experience so far from dealing with this Auckland outbreak, further support elimination as the most effective and equitable strategy response to the COVID-19 pandemic.
To prepare better for future outbreaks, there needs to be an urgent review of pandemic response measures to protect the health and wellbeing of children and young people, together with their families and teachers. COVID-19 children’s leads should be integrated into all Government agencies directing the pandemic response, with Māori and Pasifika representation in decision-making for children at every level of the response.
APPENDIX:
Reasons to be concerned about COVID-19 in Aotearoa NZ if elimination fails
Previous and current experience of childhood infectious diseases in Aotearoa paints a troubling picture of heavy burden of morbidity and mortality in the presence of powerful drivers of health inequities.
We have previously reported on the high incidence and inequities in infectious disease hospitalisations11 and mortality12 in children. The high prevalence of poor-quality, crowded housing is an important driver of outbreaks of close-contact infections, eg, meningococcal disease.13 In addition to the burden of acute infectious diseases, and uniquely in the OECD, NZ still has ongoing incidence of rheumatic heart disease, a preventable and life-limiting post-infectious condition that is now almost entirely limited to Māori and Pasifika children and young people.14
Comorbidities such as chronic lung conditions and obesity are more prevalent in Māori and Pasifika populations, and these underlying conditions are known to increase the severity risk of COVID-19. Investigations of seasonal influenza demonstrate the ‘syndemic’ impact of infectious disease in combination with multi-morbidity.15 This risk is particularly a concern for Māori and Pasifika families who are more likely to live in intergenerational households with high levels of crowding, making it difficult to protect one another from transmitting close-contact infections.
Taken together, these factors indicate a substantial risk that an uncontrolled COVID-19 outbreak would have heavier impacts on children and young people in NZ than in other high-income countries. As seen in the current outbreak, Māori and Pasifika are likely to be particularly at risk.