Summary
Nearly three New Zealanders die from accidental drug overdose every week, a preventable cause of death that disproportionately affects Māori. Fatal accidental overdose has complex, multifactorial causes, including characteristics of the illicit drug supply, individual circumstances, and social and structural factors like housing instability and economic hardship.
Reducing overdose deaths requires a suite of interventions that address these factors. Good Samaritan overdose laws (GSLs) provide legal protections to people seeking emergency help during an overdose, addressing a key situational risk factor. Local evidence shows that fear of legal consequences delays help-seeking and contributes to preventable deaths. International evidence on GSLs is mixed but consistently points in a positive direction.
Introducing GSLs, alongside other harm reduction measures, offers a meaningful, evidence-informed step toward reducing overdose deaths. The Health Select Committee is currently considering such a law through the Drug Overdose (Assistance Protection) Legislation Bill. Submissions are open until 16 June 2026.
Fatal accidental overdose is a preventable cause of death, and yet nearly three New Zealanders per week die from it. One intervention that could reduce such deaths is Good Samaritan overdose laws (GSLs) that work by removing criminal penalties for low-level drug offences when emergency help is sought during an overdose. The Drug Overdose (Assistance Protection) Legislation Bill is currently being considered by the Health Select Committee.
This Briefing describes the evidence behind GSLs and their potential impact on reducing overdose deaths.
Fatal accidental overdose in Aotearoa New Zealand
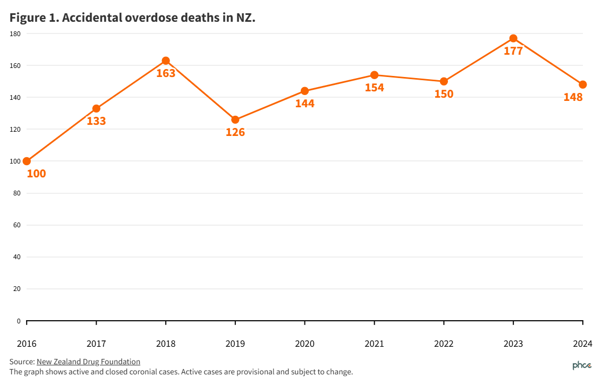
According to a NZ Drug Foundation report, 1,295 people died of accidental drug overdose between 2016 and 2024, including 148 deaths in 2024 in Aotearoa New Zealand (NZ)1. Concerningly, the annual number of fatal overdose cases has appeared to follow an upward trend since at least 2016 (Figure 1). In NZ, the population rate of fatal overdose among Māori is 2.8 times higher than among non-Māori.
Non-fatal overdose numbers appear to have been relatively stable over the last decade. Between 2015 and 2024, 6,059 people were seen in hospital due to drug poisoning. For fatal and non-fatal overdoses, opioids are the substance class that is most involved in these cases, and mixing several depressants (such as benzodiazepines or alcohol) with opioids is a common finding in fatal cases.
Preventing fatal overdose
Several factors contribute to the risk of fatal overdose among people who use drugs. In Appendix 1, we provide clarification about defining and monitoring ‘accidental overdose’. In Appendix 2, we present factors involved in the risk of fatal overdose and some interventions that can reduce the fatalities. All these interventions should be considered as part of a comprehensive programme to reduce the number of fatal overdoses. Here, we focus on GSLs because there is currently an opportunity to implement this specific measure.
Do we need GSLs in NZ?
GSLs provide legal protections for people who seek emergency help during a drug overdose. In most circumstances, the person experiencing an overdose would not be able to call for help themselves due to the effects of the drug and would require the assistance of witnesses to survive. While details vary between jurisdictions, under these laws, the caller, the person experiencing an overdose, and/or people at the scene are protected from prosecution for certain offences (typically low-level drug offences, like drug possession) if they call for help. The rationale for these laws is that fear of prosecution reduces the likelihood of emergency help seeking, so removing these concerns will result in more timely calls.
There is evidence that communities who may witness an overdose in NZ are concerned about calling emergency services. A 2025 survey of people at risk of drug harm found that 39.6% would be worried to call 111 if someone had an adverse reaction to illicit drugs.2 There is also coronial evidence that hesitancy to call has contributed to preventable overdose deaths (Table 1).
Table 1: Selected publicly available coronial case reports involving overdose and call hesitancy (in chronological order)
| Case | Description |
|---|
| Kidwell [2021] NZCorC 3 | Coroner “dumbstruck by the lack of action taken to assist [the person who experienced the overdose] by others” when he was found incapacitated. |
| Pita [2023] NZCorC 39 | Coroner noted an expert emergency doctor’s cautioning “against an approach that penalises users. Penalising users can create a barrier to seeking medical attention, even in cases of emergency.” The Coroner also highlighted the imperative for non-delay in seeking assistance. |
| Eble [2024] NZCorC 65 | Coroner noted that the person’s fiancée considered calling an ambulance several times but ultimately did not. |
| Gunnell [2024] NZCorC 156 | A young man suffered severe distress following ingestion of a hallucinogenic drug, which ultimately led to him falling off Auckland’s Symonds Street overpass. The Coroner endorsed the recommendation of a “Buddy system” through which peers can support one another and call for help in case of distress under the influence of drugs. Such a system would greatly rely on the legal certainty of non-prosecution of the person assisting or the individual experiencing an adverse drug reaction. |
| Strongman [2024] NZCorC 204 | Coroner noted the delay of a group of friends to call the services, which likely led to the person’s death. |
International evidence for GSLs
Some US studies have shown a 10–15% reduction in opioid overdose deaths within one to two years post-implementation.3,4 While the context of the drug supply and prevalence of opioid use are different in the US, applying these numbers in NZ could mean that 15–23 lives are saved each year.
One US study found the effects to be stronger among Black and Hispanic communities, with a 26% reduction in the incidence of fatal opioid overdose.3
A New York study found that following the enactment of a GSL, the number of hospitalisations for heroin overdose rose, indicating that people experiencing an overdose were more likely to receive medical care, as the law intended.5
There are still research gaps and the effects sometimes fail to reach statistical significance (see Appendix 1 for more information). Though they consistently point in a positive direction, some studies have shown mixed results with limited or no effects.6,7
Some of the limited effects of GSLs in policy research can probably be explained by their scope and the characteristics of the environments in which they function. In many jurisdictions, people who use drugs are not aware that these laws exist or how they work.8 Even if people are aware, they may lack confidence that these protections will be respected – especially if they have had previous interactions with law enforcement.9
Research has found offering comprehensive protections and explicitly removing the risk of arrest is likely to increase the effectiveness of GSLs.4 Evidence suggests that – especially for people with prior criminal justice involvement – increasing the scope and coverage of protections is likely to result in increased effectiveness of GSLs.10
We found no evidence of GSLs having unintended consequences like incentivising people to take more risk with substance use, or GSLs being used to pervert the course of justice for serious crimes.
Implementing GSLs to reduce overdose mortality in NZ
It appears that ensuring a broad scope of protections and high level of awareness are likely to improve the effectiveness of GSLs. Given the existing research gaps, it is important that the impacts of the new law are evaluated and any possible barriers to effectiveness are identified.
Coupled with other actions (eg, improving access to naloxone), GSLs could meaningfully reduce the number of avoidable deaths in NZ.
What this Briefing adds
- There are about 150 accidental overdose deaths a year in NZ with an upward trend over nearly a decade. These deaths are preventable.
- Local research with communities of people who use drugs and analysis of coronial cases demonstrate that help-seeking behaviours in the event of an overdose are hindered by fear of repercussions.
- Good Samaritan overdose laws (GSLs) work by reducing the fear of getting in trouble with law enforcement authorities among people witnessing an overdose, which may encourage seeking emergency help.
- International evidence shows that GSLs can help increase help-seeking behaviours and reduce deaths when implemented appropriately in the given environments.
Implications for policy and practice
- NZ should implement GSLs to reduce overdose fatalities. They should cover a broad scope of circumstances to ensure there is no doubt about whether they would apply.
- These protections should cover all people at the scene, and they should include a pragmatic scope of drug offences that are likely to be commonly discovered in the environments where overdoses occur. The protections should apply at all levels of law enforcement interaction, including ensuring no warrantless arrests are made in connection to the offences covered.
- It is critical that these protections apply to people with prior criminal justice involvement, and those who have had earlier interactions with the law enforcement.
- The Drug Overdose (Assistance Protection) Legislation Bill provides a mechanism to introduce a GSL into NZ.
Authors’ details
Dr Jacek Kolodziej, Policy Director, Te Puna Whakaiti Pāmaemae Kai Whakapiri | New Zealand Drug Foundation.
Michelle Judge, Policy Advisor, Te Puna Whakaiti Pāmaemae Kai Whakapiri | New Zealand Drug Foundation.
Dr Andrew Leighs, Public Health Medicine Registrar.
Dr Rose Crossin, Department of Public Health, Ōtākou Whakaihu Waka, Ōtautahi | University of Otago, Christchurch.
Professor Michael Baker, Department of Public Health, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington and Trustee Te Puna Whakaiti Pāmaemae Kai Whakapiri | New Zealand Drug Foundation
Declaration of interests
Michael Baker is a Board member of Te Puna Whakaiti Pāmamae Kai Whakapiri | New Zealand Drug Foundation.
Rose Crossin is the Chair of the Clinical Governance Committee at DISC Trust.
Appendix 1: Technical and methodological issues around classifying and monitoring overdose and interventions to prevent overdose.
Accidental overdose and self-harm incidents are distinct phenomena
In this Briefing, we only refer to the issues surrounding accidental drug overdose among people who use drugs, where it is not the person’s intention to self-harm. Intentional self-harm or suicide are distinct issues that require different services and policy responses.
Overdose surveillance and monitoring in NZ
Unlike countries such as the US, Canada, Australia or the UK, the function of monitoring fatal and non-fatal drug overdoses is not nationally coordinated in NZ. In the absence of a government system, this data is compiled and reported on by the New Zealand Drug Foundation. This information is gathered through requests made under the Official Information Act or from Information Sharing Agreements with the Crown entities that hold this information – the Office of the Chief Coroner and Te Whatu Ora.1
Measuring the impacts of harm reduction policies is challenging
Measuring the impacts of policies like GSLs is notoriously challenging. A major difficulty is the reliance on observational data and being able to account for the multiple unrelated changes that can influence the number of overdoses over time, as well as reporting and monitoring difficulties and many other factors. There are also limitations in generalising findings across jurisdictions that may have very different policy and social contexts.
Appendix 2: Selected factors increasing the risk of fatal overdose and risk mitigation interventions
| | Factor | Mechanism | Examples of interventions that can reduce the risk |
|---|
| Substance/supply-related | Opioid use | Opioids carry a risk of respiratory depression, that can be fatal with an excessive dose | Appropriate prescribing for medical conditions; provision of naloxone (an overdose reversal medication) and training about its appropriate use |
| | Polysubstance use | Combining substances, especially depressants, increases the risk of death and lowers their toxicity threshold | Provision of appropriate information about mixing substances |
| | Illicit market adulteration | Substances in the illicit market may be adulterated by unknown amounts of unexpected drugs, including potent opioids like fentanyl, or nitazenes | Drug checking; provision of naloxone and appropriate use training; safe(r) supply intervention (ie, provision of pharmaceutical grade substances to people at high risk of exposure of overdose) |
| Individual | History of non-fatal overdose | Experiencing previous non-fatal overdose is one of the strongest predictors of a subsequent fatal overdose11,12 | Treatment and harm reduction services targeted to people who have experienced non-fatal overdose |
| | Substance use disorder | Having current substance use disorder (SUD) increases the risk of fatal overdose13 through influencing the pattern of substance use | Increasing access to SUD treatment;
incorporating overdose prevention and response training in SUD treatment programmes |
| | Tolerance disruption | Following periods of abstinence, tolerance to a drug is diminished, resulting in previously tolerated doses becoming toxic. For example, this can occur in people who have been recently released from prison14 | Specific harm reduction interventions provided to people on release from custodial settings |
| Social and structural | Housing insecurity | Housing instability and homelessness15 reduce the ability to use effective harm reduction measures | Housing-first interventions that do not require abstinence as a condition for access |
| | Economic and family distress | Unemployment, economic and family distress16 create unstable environments that influence the patterns of substance use | Addressing social determinants through targeted programmes |
| Situational | Using the substance alone | Using a substance alone means that there is nobody that can monitor and give support to the person who overdoses, increasing the risk of death17 | Drug consumption sites; encouraging having someone around to monitor the person |
| | Lack of emergency response | While most fatal overdoses appear to occur in the presence of others, help-seeking is often delayed due to fear of repercussions and may arrive too late.18 The help may also not be sought by witnesses due to lack of awareness that it is occurring in witnesses | GSLs; naloxone provision; overdose response training for people who use drugs and those likely to witness an overdose; public overdose awareness programmes |