The first Delta-variant outbreak in the community brings a new challenge to Aotearoa New Zealand’s COVID-19 response. A Delta outbreak was in some respects a likely scenario given the high infectiousness of this variant and the emerging evidence that vaccines may be less effective at preventing Delta transmission compared with the original strain of the pandemic virus. In this blog we discuss public health responses employed in other jurisdictions in response to the Delta variant that may be beneficial in controlling the current Delta outbreak in NZ and strengthening NZ’s COVID-19 response in future.
We have written several blogs about different ways that NZ could improve its COVID-19 response, such as increasing wastewater testing, wider mask use, more targeted vaccinations, a revised pandemic plan[1], revisions to the Alert Levels and improvements to ventilation management. There is also a need to strengthen border control measures. Some of these past recommendations have been used in the current outbreak response, such as using region-specific Alert levels (now implemented with the ‘south of Auckland’ Alert Level split), mandating QR scanning at essential services under Alert Level 4, and suspending new bookings in MIQ facilities to free up spaces for community cases. However, with NZ nearly two weeks into its first COVID-19 Delta outbreak in the community, we should be learning from other countries’ Delta outbreak responses to inform current and future public health measures in NZ.
Why is the Delta variant such a concern?
The Delta variant (B.1.617.2, originating in India in October 2020) has become the dominant strain of COVID-19. This variant produces a much higher viral load in the upper airways contributing to it being more infectious and having a shorter incubation period.[2] Its dominance is facilitated by its high reproduction number (Ro), estimated at between 5 and 7[3] meaning that on average, a Delta case may infect between 5 to 7 other people (much higher than the original strain Ro=2.79[3] or even the Alpha variant with Ro=4-5). To put this into perspective, the Delta variant has a higher reproduction number than many other viral infections such as influenza (Ro=1-3) or Ebola (Ro=2),[4] but is not as high as chicken-pox (Ro=10-12) or measles (Ro=12-18).[5] A further selective advantage is Delta appears more resistant to vaccines, i.e. reduced efficacy of vaccination at preventing infection and transmission.[6] Its impact is further increased because Delta appears to cause more serious illness with increased hospitalisation risk[7, 8] and risk of death.[9] Therefore, NZ’s control of COVID-19 in response to this Delta outbreak and its ability to continue pursuing an ‘elimination strategy’[10] is being put to the test.
What’s the situation in Australia?
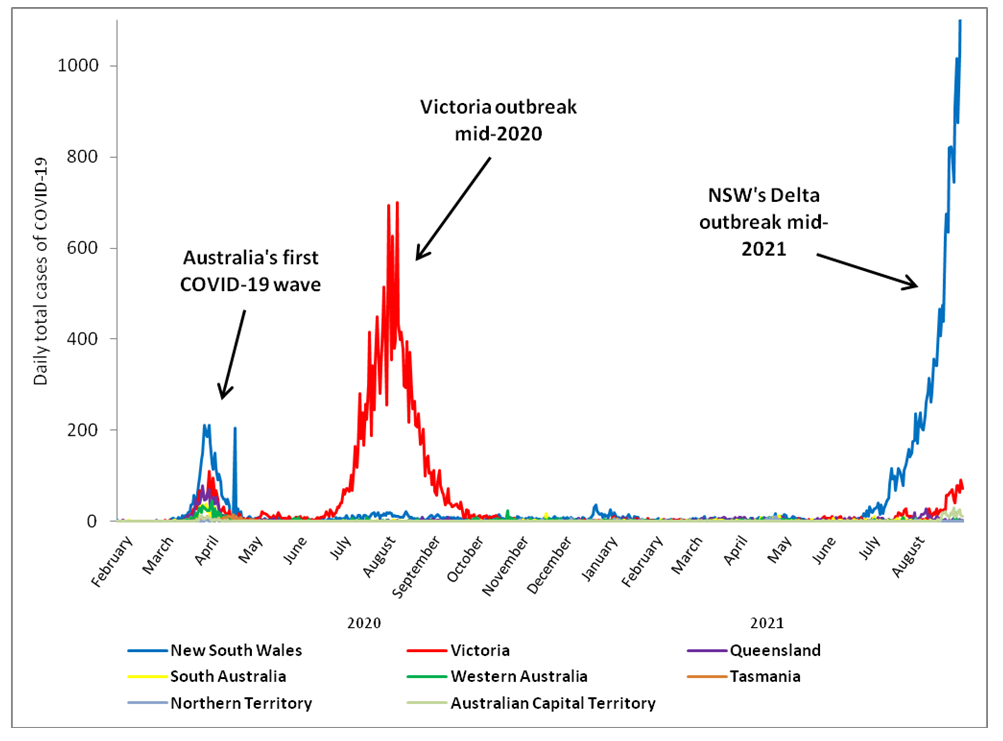
As we described in a previous blog, New South Wales (NSW) (and indeed wider Australia) is tackling it’s largest outbreak in the COVID-19 pandemic. The Delta variant is fuelling this outbreak, with nearly 1400 cases in Australia reported on 30 August 2021 (a new record for daily cases) (figure 1). Even with various state border restrictions with NSW, this outbreak has spread into other Australian states/territories and NZ (i.e. Victoria [experiencing a high number of cases amongst children] and Australian Capital Territory). The delay to implement an initial strict lockdown within the greater Sydney region has arguably resulted in a prolonged outbreak, and has put serious pressure on Sydney’s health system.
Figure 1: Daily total COVID-19 cases in Australia up to 30 August 2021 (data from www.covid19data.com.au)
Queenslanders have experienced a range of snap lockdowns in response to various Delta outbreaks in the last several weeks. These lockdowns tend to be very strict and imposed with short notice. For example in late July, a Delta outbreak in Brisbane (which was reported to be widely driven by school children) resulted in a strict lockdown the following day. Queensland has managed to reduce the number of reported COVID-19 cases in the state to less than 10 per day for the last two weeks. However, Queenslanders have been warned that with Delta COVID-19 cases linked to the NSW outbreak getting closer to the Queensland’s border, authorities expect that cases will inevitably jump the border.
Queensland’s border restrictions with NSW will stay in place until at least October, with the Queensland Health Department stating that “this is based on the timeframe in which we hope to have 70 per cent of Queenslanders fully vaccinated against COVID-19”. As of 25 August 2021, capacity issues with the quarantine hotels has meant a pause on entry to Queensland for those who have travelled from a pandemic hotspot. Queensland Premier Annastacia Palaszczuk announced on 26 August 2021 that given the limitations of hotel-based quarantine (i.e. capacity, design and location and in particular the Delta variant), Queensland has begun building its own dedicated regional COVID-19 quarantine facility with 500 beds. The Premier in her announcement mentioned the success of the Howards Springs Facility in Northern Territory as a dedicated COVID-19 quarantine facility.[11]
South Australia has experienced a relatively low COVID-19 case load, with daily cases not reaching double-digits since June 2021. A state-wide snap lockdown in July enabled South Australia to keep the Delta outbreak in the community from spreading widely. This lockdown was similar to an Alert Level 4 in NZ and given the situation in NSW at the time, it was widely feared that there would be a surge in community cases. However, South Australia has continued to kept Delta out of the community, and is currently under ‘Activity Restriction Level 1‘, which places some restrictions on physical distancing, mask use and food/drink retail facilities (somewhat a mix of NZ’s Alert levels 1 and 2).
Tasmania, Western Australia and the Northern Territory have all recently had no or few reports of community cases of COVID-19. Tasmania, being an island state has geographical advantages for keeping the Delta variant out of its population, however officials are still planning for a Delta outbreak scenario. Referred to as a “Delta Shield”, it would involve a quickly implemented lockdown (either a specific region or state-wide) and mandated public health measures such as gathering restrictions and mask use. Both Western Australia and Northern Territory have experience with the Delta variant and both have had various lockdowns in response to community cases. The ongoing outbreak(s) of the Delta variant throughout many states/territories in Australia have now cast doubt upon Australia’s ‘aggressive suppression’ COVID-19 strategy going forward.
How are other jurisdictions responding to Delta?
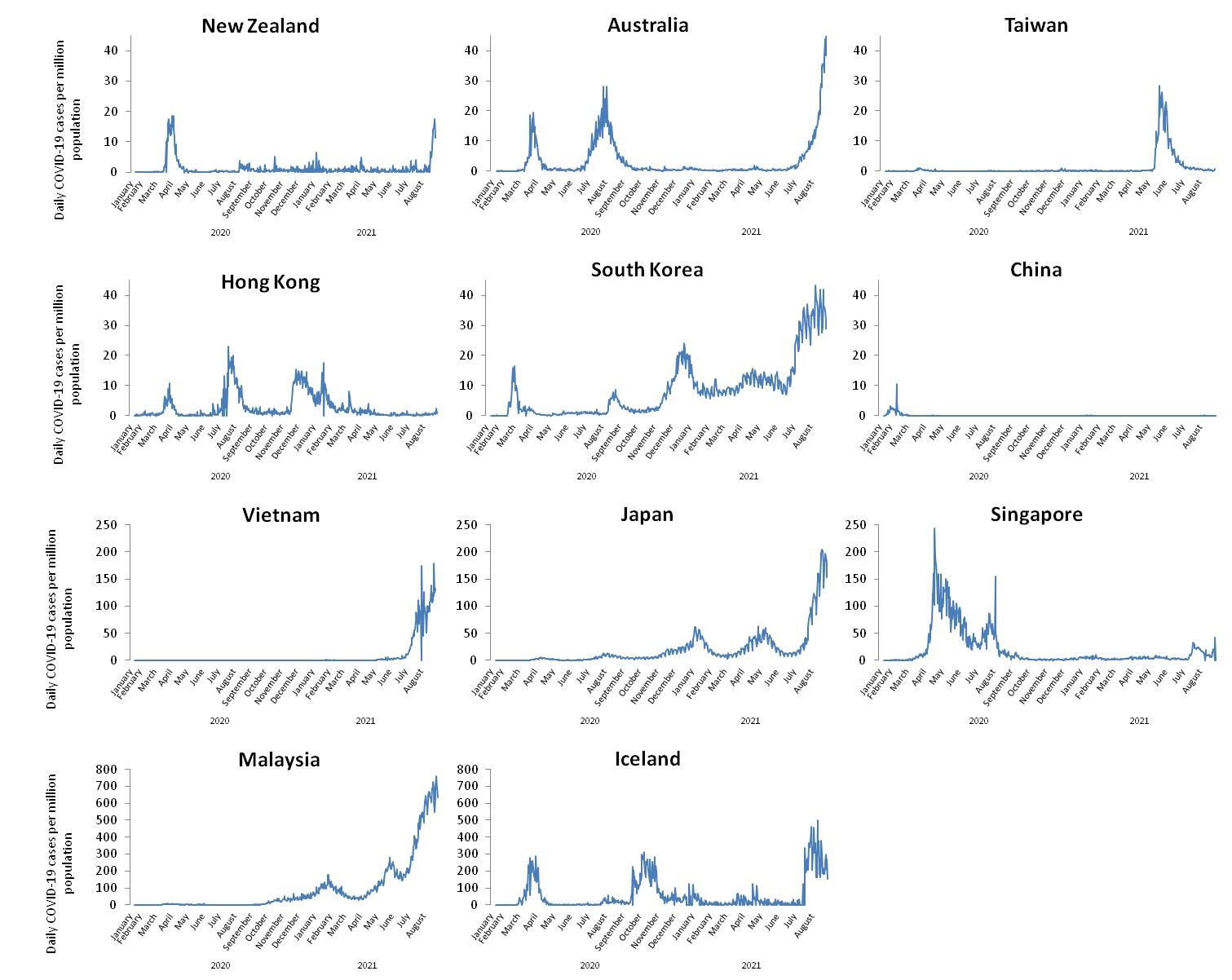
Taiwan was often cited in 2020 as a model jurisdictions in terms of its response to the COVID-19 pandemic.[1] But in April 2021 Taiwan experienced its biggest COVID-19 outbreak, first identified as being caused by the Alpha variant, with the Delta variant later identified at the tail-end of the outbreak resulting in localised lockdowns. Notably, Taiwan has still not implemented a full-strength nation-wide lockdown in response to COVID-19. However, Taiwan appears to have succeeded with outbreak control and has reported zero cases in the community by late August 2021 (see graph in the Appendix).
Many other Asian jurisdictions are now tackling Delta outbreaks with varying success and failure (see graphs in the Appendix).[12] For example, Malaysia, Japan, South Korea and Vietnam are experiencing record numbers of cases as they grapple with both Delta along with other COVID-19 variants (figure 3). It is worth noting that along with Taiwan, some other nations also appear to be successfully combating Delta outbreaks. For example, Singapore (soon to be moving away from a “zero-tolerance” approach to COVID-19) and China (using a mixture of localised lockdowns/restrictions and mass testing) are all experiencing daily case decreases in their respective recent outbreaks predominantly caused by the Delta variant. Hong Kong, which has an elimination strategy,[13] has so far managed to avoid a major Delta outbreak. It has had reported cases, for which officials enforced localised restrictions (including compulsory testing) to restrict spread. Hong Kong is also continuing its “zero tolerance” approach to COVID-19, with tightening restrictions for incoming travellers being put in place (although vaccinated travellers have lesser restrictions).
Iceland has experienced several COVID-19 waves throughout the pandemic, but in the past was able to return to few or no cases of COVID-19 in the community. However, Iceland is now experiencing it’s largest COVID-19 outbreak caused by the Delta variant. Even though Iceland has one of the highest COVID-19 vaccination rates in the world (~84% of eligible Icelanders are fully vaccinated),[14] breakthrough infections are considered to be driving the current outbreak.
What is the relevance for NZ’s Delta outbreak?
For NZ and other nations continuing to pursue a COVID-19 elimination strategy for the foreseeable future, a community case of COVID-19 should initially be presumed to be the Delta variant given its dominance worldwide. This is the approach that the NZ Government took following the confirmation of a community case in Auckland on 17 August, unlike their counterparts in NSW. NZ should also consider following Queensland’s approach by building a specific COVID-19 quarantine facility and lessen the risk of future MIQ system failures.[11]
It is clear from other nations that a quickly implemented lockdown (whether regional or nationwide) can be effective in dealing with Delta outbreaks when coupled with extensive public health measures such as physical distancing, mass mask use and vaccination. However, officials should be aware that even high-levels of vaccination amongst the eligible population may not be as effective as hoped against COVID-19 as a result of Delta, as evidenced in Iceland. Indeed, there is a concern about loosening border restrictions when children under 12 are still not eligible to be vaccinated and the full impact of Delta infections in children remains unclear.[15] Despite these risks, some countries, notably Singapore and Australia (at the Federal rather than state and territory level) appear to be moving away from an elimination strategy and have articulated roadmaps towards what appear to be suppression approaches with COVID-19 as an endemic infection.
There are many reasons for NZ to continue pursuing an elimination approach, for at least the medium term, even with the Delta variant. Elimination will help to:
- Maintain NZ’s relatively lower morbidity and mortality outcomes. There is still limited understanding of the health effects of long-COVID, which could be quite severe.[16] Children are largely unvaccinated and would experience high rates of infection and hospitalisation in an uncontrolled outbreak.
- Prevent the severe health inequities caused by COVID-19 in NZ and elsewhere.
- Reduce/avoid health system volume overload (impacting on routine care).
- Potentially reduce adverse impacts on GDP and employment.[17]
- Protect NZ from new COVID-19 variants that may be more infectious, vaccine resistant, and lethal than even the Delta variant (as described in the SAGE report to the UK Government).[18]
- More broadly, continuing the elimination strategy in the medium term allows NZ to keep its option open.
In summary, experiences from South Australia, Queensland, Taiwan, Hong Kong, China and Singapore show that it is possible to control Delta outbreaks, although it requires extensive and swiftly implemented public health interventions. High vaccination uptake will significantly reduce infections and serious complications, but population-level immunity will be limited by the lower efficacy of current vaccines against infection and transmission of the Delta variant. Therefore, NZ should continue with its efforts to control the current outbreak, and consider strengthening the Alert Levels to account for increased transmissibility of the Delta variant. NZ should also explore new public health measures (such as improved border biosecurity and building a dedicated quarantine facility) that will aid NZ’s ongoing response to the COVID-19 pandemic and future pandemics.
*Author Details: Department of Public Health, University of Otago, Wellington
Appendix: Daily COVID-19 cases per million population in selected jurisdictions up to 30 August 2021 (data from https://ourworldindata.org/coronavirus)