Summary
Long COVID is emerging as a global public health concern. Health care workers have a relatively high level of exposure to COVID-19 and an elevated risk of Long COVID. This article describes an innovative multidisciplinary approach used for Te Whatu Ora staff with Long COVID in Taranaki. A survey of key stakeholders found that all respondents considered that the service was making a difference for people with Long COVID. Its multi-disciplinary team approach was strongly supported. Te Whatu Ora should consider funding such services more widely. Their development should draw on best international practice and careful evaluation of their effectiveness in Aotearoa.
Long COVID (post-acute COVID-19) describes a condition where people continue to suffer signs and symptoms for more than 12 weeks after their acute infection1. Some are referring to it as a new epidemic2. Health care workers have a relatively high level of workplace exposure to COVID-19 and a significant proportion of those diagnosed with COVID report sequelae such as fatigue and breathlessness many months after their infection3.
Common ongoing symptoms of Long COVID include fatigue or general malaise, headaches, cognitive impairment, attention disorders, or respiratory symptoms4. Women, older people, and people with higher BMI, pre-existing comorbidities and severe infection are more likely to experience symptoms that last longer than 12 weeks5. Research from Australia in 2022 estimates that 5% to 10% of COVID-19 cases result in Long COVID6. A recent New Zealand study of 990 participants who contracted COVID-19 before December 2021 found that 22% had symptoms which were consistent with Long COVID7.
Supporting health care workers with Long COVID
The first case of COVID-19 in a Taranaki District Health Board (now Te Whatu Ora Taranaki) staff member was reported to the Occupational Health Department in February 2022. By 10 February 2023, 2618 people had reported a new or reinfection positive COVID-19 test result out of the 2532 people employed by Te Whatu Ora Taranaki8. Te Whatu Ora Taranaki (TWO Taranaki) staff with persistent symptoms started to seek support from physiotherapy and occupational therapy colleagues on an ad-hoc basis from March 2022.
The Taranaki Long COVID clinic was developed for staff by the Physiotherapy, Occupational Therapy and Occupational Health Departments in May 2022, modifying existing pathways. Steps taken included building a process using national and international guidelines9-15 and inviting contingent allied health professionals to participate. This required considerable lobbying and education.
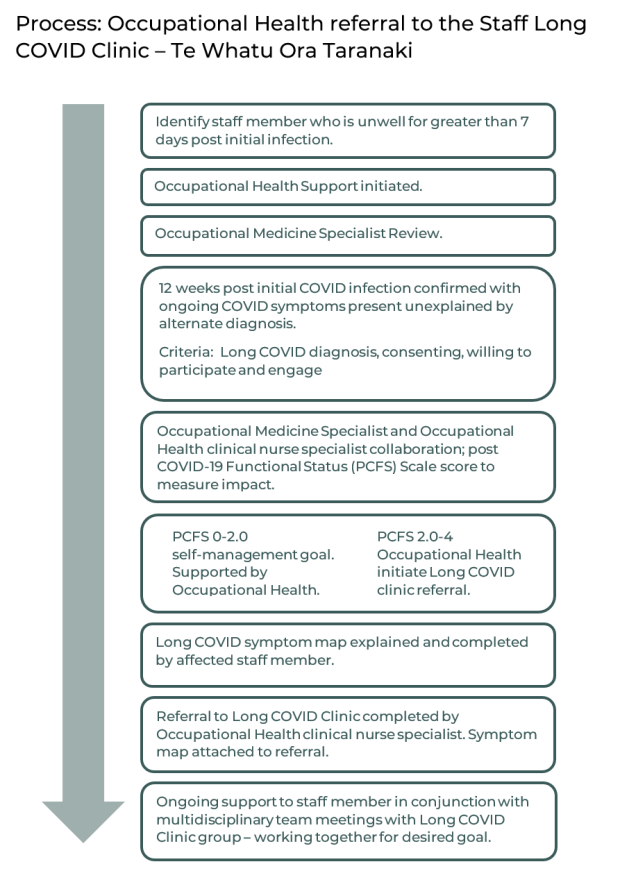
Operation of the service is based on following-up staff with COVID-19, 12 weeks post-infection, with an interview by occupational health staff. The impact of the disease is measured using a post COVID-19 Functional Status Scale16 - see figure below. If there is mild impairment, a self-management strategy of care is employed; if there is moderate to severe impairment then targeted or personalised care is provided. A Symptom Map17 is completed to identify an individual’s specific cluster of symptoms and directs referrals to the specific allied health professional/s required. Continued collaboration with national and international groups has ensured that the service is offering an appropriate response. Currently the service does not receive dedicated funding and most of the time spent developing the service and creating resources occurred voluntarily in personal time.
A review of patients seen by the Long COVID clinic showed that 18 TWO Taranaki staff were enrolled between 11 June 2022 and 10 February 2023. All were female and the mean age was 51 years (range 37-65 years). The majority were New Zealand European (14/18), two were Māori ethnicity (2/18) and two were “Other” ethnicities. The number of people enrolled with the service was 0.7 percent of the total TWO Taranaki workforce8.
How key people perceive the Long COVID service in Taranaki
A SurveyMonkey questionnaire on perceptions of the programme was sent to 15 key stakeholders including members of Allied Health Team, physicians, referrers and managers during January 2023. The survey was completed by nine people. Responses were anonymised, see Appendix One below.
Eight of the nine respondents were in agreement that the Long COVID clinic for staff was meeting patient needs and all considered that patients had improved because of the service. All respondents considered that the multi-disciplinary team approach involving allied health and occupational health was the main strength of the service. In contrast eight of nine respondents felt that lack of resources, funding and capacity were the main weaknesses of the service. Despite the largely unpaid contributions to the development of the service which at times were “exhausting and demanding”, several people noted the appreciation and positive feedback from staff that they were seeing.
Most of the people I see are just like me - working full time and have busy active lives. They will often say to me “I've just got nothing in the tank”; “my battery pack has died”; “even my wairua - everything is affected”. Everyone I have seen has been so thankful to receive validation of their symptoms. Respondent #6.
This evaluation of the Long COVID Clinic in Taranaki has highlighted the perceived strength of the multidisciplinary approach by stakeholders which uses international best practice to respond to an unmet health need. Health care workers face an elevated risk of acute COVID-19 compared with the general population (probably due to occupational risk) and the burden of Long COVID is likely to be large2,18,19. However, health care workers also tend to be reluctant to seek care for themselves19 and for this reason it is likely that there are staff in Taranaki with ongoing symptoms who have not accessed the Long COVID clinic. Currently less than one percent of the infected workforce have enrolled with the service.
In Australia Long COVID clinics have been set up in several locations to provide specialist care to people having long term symptoms6. This has not happened in Aotearoa New Zealand and academics have warned that the health sector is letting down people who experience symptoms of Long COVID20. We recommend that Te Whatu Ora recognises the burden of this seemingly neglected disease and appropriately funds services for people who are likely to have acquired Long COVID through their work – rather than relying on the goodwill of health professionals working in their spare time.
“Simply put, the health and wellbeing of New Zealanders depends on the health and wellbeing of healthcare workers.” 21
What is new in this Briefing
- An innovative Long COVID clinic in Taranaki is presented as a case study of supporting health care workers.
- A survey of key stakeholders found that all respondents considered that the service was making a difference for people with long COVID and that the multi-disciplinary team approach involving allied health and occupational health was its main strength.
- It is likely that the Long COVID clinic is under-utilised as health care workers tend to be reluctant to seek care for themselves.
Implication for public health practice and policy
- Te Whatu Ora should consider funding services for people who acquire Long COVID through their work rather than relying on the goodwill of health professionals working in their spare time.
- As this was a small initial evaluation, larger evaluations are needed for Long COVID services in Aotearoa New Zealand, along with regular updates of guidelines that reflect international best practice in managing Long COVID.
Author details
Dr Shereen Zaidi was a TWO-Taranaki house officer on a public health run at the time the study was undertaken.
Fiona (Fy) Dunford is a Senior cardiorespiratory physiotherapist at TWO-Taranaki
Dr Jonathan Jarman is a public health medicine specialist and former Medical Officer of Health in Taranaki.
No competing interests declared
Acknowledgements
Cardiorespiratory Special Interest Group Committee Members (Physiotherapy New Zealand); Long Covid Staff Clinic Tier 1 team: Occupational Health: Lauren Piercy. Occupational Therapy: Rachael Grady. Physiotherapy, Zoe Manderson. Speech Language Therapy, Julia Culliford; patients attending Long COVID clinic TWO-Taranaki; Dr John Kerr and Prof Nick Wilson.
APPENDIX ONE – Summary of main feedback from stakeholders on Te Whatu Ora Taranaki Long COVID staff clinic with selected comments.
Question 1. Please select the option below that aligns with your view on the following statement: The Long COVID staff clinic is meeting patient needs. (n=9) | | |
| Strongly agree | 1 | 11% |
| Agree | 7 | 78% |
| Neither agree nor disagree | 1 | 11% |
| Disagree | 0 | 0% |
Strongly disagree | 0 | 0% |
Question 2. Do you think patients have improved through using this service? (n=9) | | |
| Yes | 9 | 100% |
No | 0 | 0% |
| Question 3. How have you seen patients improving because of this service? Please tick all that apply. (n=9) Respondents were able to tick more than one answer. | | |
| Return to work progression | 6 | 67% |
| Documented feedback from patients | 5 | 56% |
| Change in symptom map scores (subjective) | 4 | 44% |
| Change in specific validated objective measures | 4 | 44% |
| Post Covid Functional Status Scale (PCFS) impact score improvement | 3 | 33% |
| Not applicable (I am not actively treating patients with Long COVID at present) | 2 | 22% |
| Other | 3 | 33% |
| Question 4. Briefly tell us what are the main strengths of this service. (n=9). Respondents were able to volunteer more than one strength. | | |
| Multi-disciplinary team (MDT) approach; team work and collaboration with different departments | 9 | 100% |
| Evidence-based practice; best practice using validated tools based on international models | 4 | 44% |
| Selected response: “Group of health professionals working interdisciplinary to provide best practice with limited FTE they have.” Respondent #7 | | |
| Question 5. Briefly tell us what are the main weaknesses of this service. (n=9). Respondents were able to volunteer more than one weakness. | | |
| Lack of funding, resources and FTE; lack of capacity | 8 | 89% |
| Reliance on volunteer hours and unpaid time | 4 | 44% |
| Learning as we go – pathways are still needing to be developed; evolving | 3 | 33% |
| Inability to see community/outpatient referrals | 3 | 33% |
| Selected response: “Lack of FTE allocation placing constraints on staff, equity with other clinical responsibilities/caseloads. Significant work and service development performed in unpaid time. Service developed through staff ‘goodwill’ and bottom up pressure. Narrow range of MDT professions are actually providing face to face service - no community Social Work exists for example, Health Psychology scarce resource. Lack of clear lines of consistent communication and management as multi-professional peer led service - evolving.” Respondent #8 | | |
| Question 6. Do you have any suggestions to improve this service? (n=9) | | |
| Dedicated FTE and funding | 6 | 67% |
| Needs based resourcing | 2 | 22% |
| Wider multi-disciplinary team | 2 | 22% |
| Selected response: “Long COVID is an accepted condition that does well with the right support. With better resourcing, more self-management strategies via online and primary health would help meet demand, saving finite resource use for those with higher symptom impact. We should continue to promote the effectiveness of the symptom lead response and look at overseas examples, including Australia to support staff and public with Long COVID.” Respondent #6 | | |
| Question 7. Do you have any other comments or memorable moments to share? Selected responses: | | |
| “Our small service has made a huge difference to staff members with COVID – we are trying now to provide a service to the public but we are very limited due to no resourcing of the team.” Respondent #3 | | |
| “Very proud of all staff involved in this project they have done an amazing job.” Respondent #7 | | |
| “This new piece of work is exhausting and demanding but we have chosen to be a part of it voluntarily. The appreciation and positive feedback from the staff we are seeing is hugely humbling and motivating. They have been so positive and open to the education and input we have provided they have in some cases acted as the next tier of devolving these important messages and copied and handed on information sheets. Spreading the advice and support further amongst our wider workforce, caring for each other.” Respondent #8 | | |