The global outbreak of monkeypox has for the first time caused widespread transmission outside African countries where it is endemic. Aotearoa New Zealand (NZ) had its first case diagnosed on Saturday 9 July 2022. This outbreak currently represents a relatively low public health risk to NZ because, while potentially transmissible here, spread is easily contained with case isolation and contact management. However, this outbreak could become an important global health threat for low- and middle-income countries. NZ should consider supporting health initiatives to control this infection in countries where it is an endemic zoonotic disease, and in other countries to eliminate it, including in NZ itself.
We are experiencing a global outbreak of monkeypox which has for the first time caused widespread transmission outside African countries where it is endemic. The outbreak has spread to 57 countries which now include Aotearoa New Zealand (NZ) following the diagnosis of our first case on Saturday 9 July 20221.
The Covid-19 pandemic has illustrated the importance of having a highly systematic approach to developing and delivering an effective response to emerging infectious disease threats2. We have previously proposed a comprehensive framework to guide the response to an emerging infectious disease risk based on effective risk assessment and management. Here we apply that approach to the monkeypox outbreak.
Global monkeypox spread and status
Monkeypox is endemic to several African countries, including Democratic Republic of the Congo, Nigeria, Cameroon, and the Central African Republic where outbreaks are currently occurring. The disease is a viral zoonosis which can infect multiple animals, though the reservoir and ecology are not well understood. It occurs in two clades, with the West African clade reported to cause less severe disease in humans (case fatality risk [CFR] = 3.6%) compared with the Congo Basin clade (CFR = 10.6%).
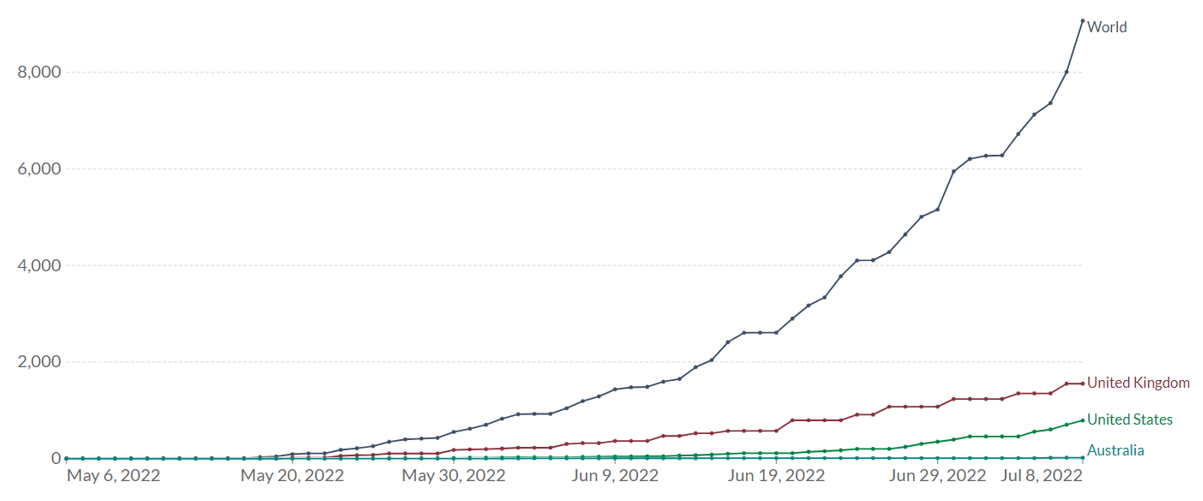
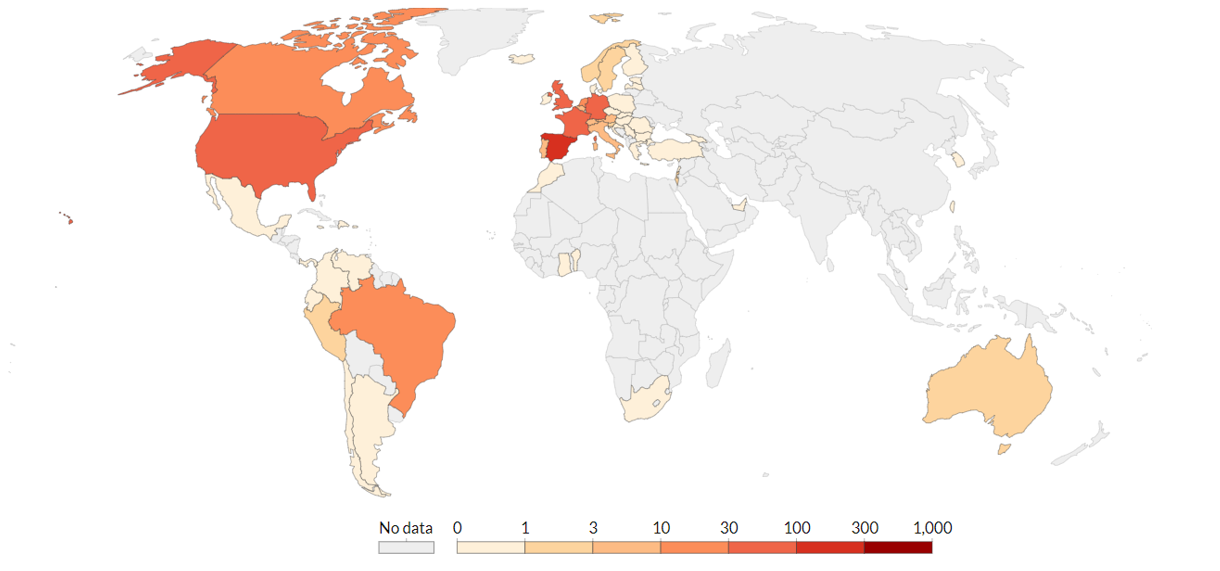
The global monkeypox outbreak is highly unusual. As of 8 July 2022 there are 8238 confirmed cases in 57 countries, territories, and areas1. Case numbers (Fig 1) and the geographic spread (Fig 2) are increasing steadily. Technically it could be termed a pandemic, as it is an outbreak that has spread to multiple countries, though that term does not have a precise definition in international law. Instead, the key designation under the International Health Regulations is “Public Health Emergency of International Concern” (PHEIC). This is an event that may “potentially require a coordinated international response.” The WHO Emergency Committee met in June and concluded that this outbreak did not yet meet the criteria to be designated as a PHEIC3. However, it plans to reconvene a meeting of its Emergency Committee in mid-July to review this decision.
Figure 1. Cumulative Confirmed Monkeypox Cases in 2022 Outbreak
Source: Our World in Data. Edouard Mathieu, Saloni Dattani, Hannah Ritchie and Max Roser (2022) – “Monkeypox”. Published online at OurWorldInData.org. Time span: 12 May 2022 to 08 July 2022. Data extracted: 10 July 2022.
Figure 2. Geographic Spread of Daily Confirmed Monkeypox Cases in 2022 Outbreak
Source: Our World in Data. Edouard Mathieu, Saloni Dattani, Hannah Ritchie and Max Roser (2022) – “Monkeypox”. Published online at OurWorldInData.org. Time span: 12 May 2022 to 08 July 2022. Data extracted: 10 July 2022. Note: This figure does not include one monkeypox case identified in NZ on 9 July 2022.
Monkeypox symptoms and transmission
Monkeypox is an infection caused by the monkeypox virus which is part of the Orthopoxvirus genus in the family Poxviridae4–6. The virus is closely related to the smallpox virus yet causes a comparatively milder course of infection4–6. Initial symptoms appear about nine days after exposure and can include headache, fever, muscle aches, fatigue, and swollen lymph nodes5,7–11. A characteristic rash that spreads over the body can develop concurrently or after initial symptoms develop. Rashes usually begin on the face and can spread to the arms, legs, chest, hands, soles of feet, and mucous membranes such as the inside of mouth, nose, eyes, anus, and genitalia5,7,8,12,13.
Secondary complications of initial monkeypox infection identified in prior outbreaks include encephalitis, sepsis, bronchopneumonia, and infection of the cornea leading to vision loss, and in some outbreaks complications have been seen in up to a third of cases5,14,15. Clinical data from 34 cases in the 2003 United States monkeypox outbreak showed additional complications such as multiple abnormal laboratory findings, cervical lymphadenopathy, and high ICU admission rates for paediatric patients16.
Recent outbreaks of monkeypox infection show an increase in human-to-human transmission12,17. The present known routes of human-to-human transmission are skin-to-skin contact, contact with clothing, bedding, or towels of an infected person, and breathing in respiratory droplets from an infected person5,6,10,12,13,17,18. While monkeypox is not a sexually transmitted infection (STI), it can spread during sexual activity as the virus spreads through skin-to-skin contact7,13. Individuals with high levels of close contact interactions are at heightened risk for monkeypox infection. This includes, but is not limited to, frontline health care workers, hospitality workers, children, and household members and partners of infected individuals.
Risk assessment for monkeypox in Aotearoa NZ
The following factors are critical in the evaluation of an emerging pandemic disease2:
Transmissibility: This characteristic indicates the potential to infect a large proportion of the population. Monkeypox is moderately transmissible in some situations. The basic reproduction number (R0), which is the number of cases each case will typically infect, has been estimated at 2.1319. On that basis the infection could spread widely unless control measures are applied. There is a wide range of potential scenarios.
Severity: This measure includes acute and long-term morbidity and mortality as well as inequalities in its impact. The case fatality risk in recent outbreaks in Africa has been 3.6% to 10.6% depending on the infecting clade of virus. Higher rates of severe infection and fatality have been seen in children and immunocompromised individuals5,12.
Controllability: This factor indicates the need for additional controls over and above standard infectious disease control measures that are currently in place. Monkeypox is considered relatively controllable because infectious cases have symptoms and the incubation period is relatively long (usually 6 to 13 days), allowing time for effective contact tracing. Known close contacts of confirmed and suspected cases identified through contact tracing can be given smallpox vaccines to stop forward transmission20,21. This method of vaccination is known as ring vaccination and has already been implemented in several affected countries20,22.
Level of uncertainty: This criterion relates to how well-characterised and stable the threat is assessed to be. A key question with the current outbreak is whether the virus has changed from previous circulating strains. The lineage of monkeypox identified in the United Kingdom has a number of genome mutations of medium to high priority for investigation. These mutations indicate possible increases in disease severity and fatality risk as compared with previous strains of the virus, along with changes to the target site of antiviral Tecovirimat which may reduce its efficacy23.
Risk management for monkeypox in Aotearoa NZ
Jurisdictions currently experiencing new monkeypox outbreaks are reporting undetected spread within the community, shown by a lack of known exposure source in many confirmed cases18. Several factors including the long incubation time and lack of experience with this disease can contribute to reporting and diagnostic delays 4,11. However, there is a strong foundation of expertise and experience in countries where monkeypox has been endemic for many years.
The framework for emerging pandemic diseases response suggests the following broad approaches2
1. Identify the high-level pandemic management strategy
The risk assessment shows that it is important to prevent monkeypox from becoming an endemic disease in NZ. The disease is also highly controllable. Consequently, it is reasonable for NZ to adopt an elimination strategy for monkeypox, rather than suppression or mitigation. This is a contrast with the current strategy settings for Covid-19 and seasonal influenza.
2. Implement case-based controls
Eliminating monkeypox requires a case-based approach, which seeks to identify all cases and interrupt further transmission from them. NZ has already taken the initial step by making monkeypox a notifiable condition to expedite case identification and reporting by health practitioners.
The NZ Ministry of Health – Manatū Hauora – has created clear and accessible public communication about monkeypox to facilitate public understanding of the infection and promote healthcare-seeking should individuals develop symptoms. Communications should be developed to be culturally appropriate and use a variety of languages. However, the information for clinicians on the same website needs to be updated. For example, now that NZ has identified a local case, PCR testing may be warranted for those who meet the clinical but not epidemiological criteria.
It is imperative for all cases to be identified quickly to break the chain of transmission and avoid misdiagnosis that would allow continued community spread. NZ can use its existing infrastructure of contact tracing and viral genome testing (as developed during the current Covid-19 pandemic) to track community outbreaks.
Suspected and confirmed cases should isolate in their homes or in government-provided isolation facilities until they have recovered. Support, such as financial, medical, and food supplies, should be provided to those isolating due to infection. Quarantine of healthy contacts is not currently recommended but they should be monitored for symptoms for 21 days after their last exposure.
Smallpox vaccine could be considered for use to vaccinate close contacts of confirmed cases of monkeypox (ring vaccination). This strategy has been implemented in some affected countries20,22,24.
3. Implement population level prevention measures
Although the main focus should be on case management, population-level measures could be useful to lower the risk of New Zealanders getting infected with monkeypox virus. Jurisdictions experiencing outbreaks are not imposing travel restrictions, but travellers to countries where transmission is occurring should be provided with advice about how to avoid infection. Mass gatherings, eg, festivals are likely to benefit from public health engagement to ensure provision of appropriate public health messaging and hygiene facilities. The value of mask wearing outside healthcare settings is currently unclear, but prolonged viral shedding from the upper respiratory tract has been observed in monkeypox cases, indicating a need to clarify this point25. Many of the cases are men who have sex with men who have become infected through close contact at organised events in Europe11,23. Consequently, it would be important to work with organisations such as the Burnett Foundation Aotearoa to design and delivery suitable health information about both prevention measures and also the need for early case recognition and control.
4. Support an effective and equitable global health response
The monkeypox outbreak is a result of failure to manage an infectious disease at the source12,17.
The current monkeypox outbreak is a concern for global health security and the risk is highest for low- and middle-income countries. Existing resources and supplies should be distributed to monkeypox endemic areas, as source locations may not have the infrastructure for effective case and contact management 26.
There is also a potential risk that this virus could become established in animal reservoirs outside its existing range. NZ could consider providing greater support for global health initiatives to control this threat in countries where it is an endemic zoonotic disease and helping to eliminate it elsewhere. Further investment is needed in researching key questions around prevention and control of this emerging infectious disease, including its animal reservoirs and how to manage outbreaks.
Finally, NZ’s new Public Health Agency should review the monkeypox response as a test of NZ’s capability to rapidly respond to a novel infectious disease outbreak, including monkeypox’s near-relative and potential bioweapon candidate, smallpox.
*Authors: All authors are members of the Department of Public Health, University of Otago, Wellington