Summary
This Briefing updates the epidemiology of the continuing Campylobacter infection epidemic in Aotearoa New Zealand (NZ). Contaminated fresh chicken meat remains the dominant source, causing an estimated 77% of infections. A strong regulatory response in 2007 halved disease rates in three months. In the subsequent 17 years, disease incidence appears to have increased by almost 70%, based on hospitalisations. During that period, we estimate that contaminated chicken caused more than 600,000 cases of illness, over 9000 hospitalisations, at least 60 deaths, and economic costs of approximately $1.4 billion.
This ongoing epidemic demands strong industry and regulatory interventions to control the source of infection and protect the NZ public, health system and economy. Immediate measures could include introducing low allowable levels of Campylobacter on fresh poultry for sale and labelling all fresh chicken products to highlight this risk and how to minimise it. NZ also needs to reinstate an independent regulator to oversee comprehensive control measures to largely eliminate human infections from contaminated chicken.
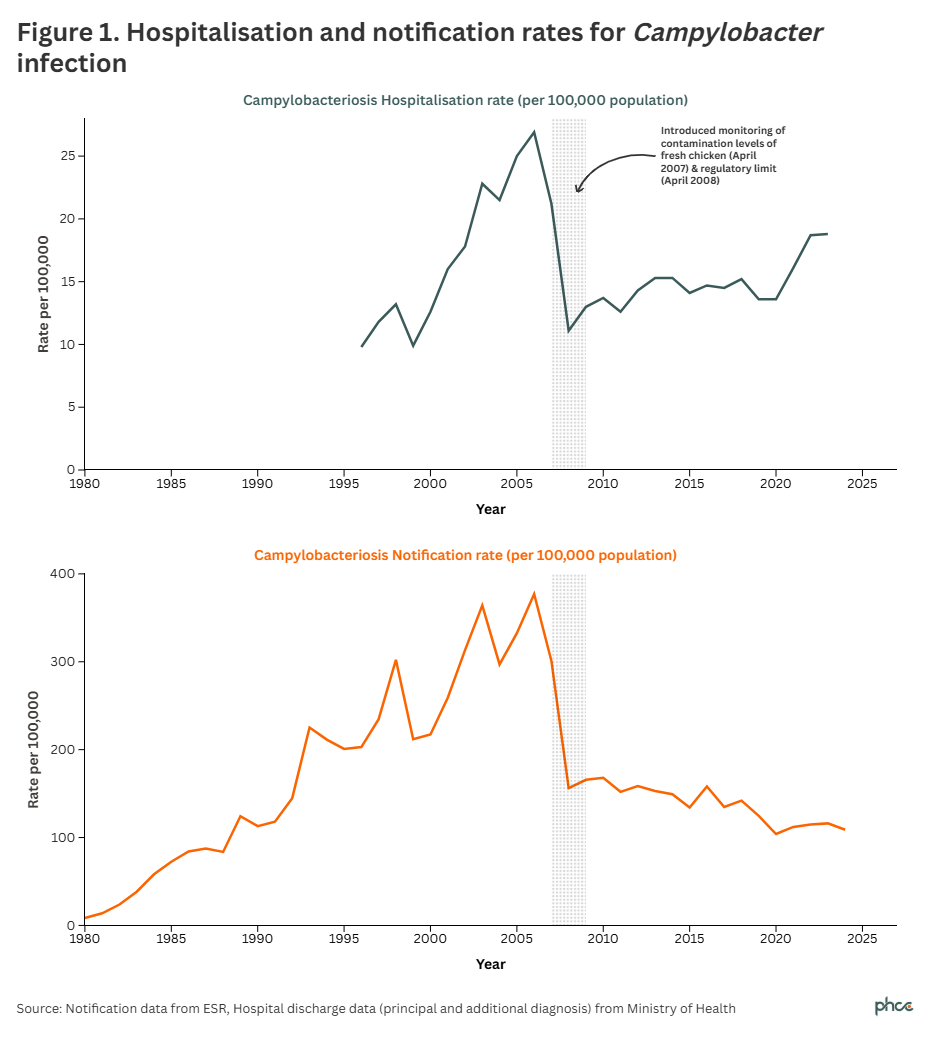
In Aotearoa New Zealand (NZ), contaminated fresh chicken meat is the largest single source of human Campylobacter infection (campylobacteriosis), and by far our most important foodborne disease threat.1 A huge increase in this infection from 1980 to 2005 paralleled the rise in fresh chicken meat consumption, hence its description as a prolonged epidemic.2 Rates of notifications and hospitalisations halved in 2007 after regulatory measures were introduced to reduce contamination levels in fresh chicken meat tested in processing plants.3 There was also a significant decline in the associated severe, and sometimes fatal, neurological condition Guillain-Barré syndrome (GBS).4
In the 17 years since the successful regulatory intervention in 2006-2007, the notification rate for campylobacteriosis declined by 30.4%, whereas the hospitalisation rate rose by 69.7% (both trends were statistically significantly at p<0.001) (Figure 1). We consider that hospitalisations provide a more robust indicator of disease trends than notifications, since the latter are more impacted by changes in healthcare-seeking behaviour and primary care access (though both would have been affected by changes in laboratory testing methods over the 2015 to 2023 period5). On balance, the rise in hospitalisations suggests a real and substantial increase in Campylobacter infection since 2008.
Contribution of contaminated chicken meat to this epidemic
Many epidemiological studies in NZ have implicated chicken meat in this epidemic.6-8 A high-quality case-control study published in 2020 found that 84% of cases were infected with strains attributed to a chicken source of Campylobacter.9 Adjusting for the proportion of cases linked to travel (8%), suggests that 77% of cases can reasonably be attributed to a chicken source.
This ongoing epidemic is the largest food safety problem in NZ and has major health and economic consequences.1 The Appendix contains a detailed assessment of the impact of Campylobacter infections since the regulatory intervention which lowered rates to a new baseline level in 2008. In the subsequent 17-year period (2008 to 2024), we estimate that contaminated chicken meat has resulted in the following impacts:
- 622,000 symptomatic cases, an average of 36,600 per year
- 85,200 notified cases, an average of 5,010 per year
- 9,100 hospitalised cases, an average of 535 per year
- 330 cases of Guillain-Barré syndrome, an average of 19 per year
- 68 deaths, an average of 4 per year
- economic costs of approximately $1.4 billion or $80 million per year.
All these estimates are subject to uncertainties which are discussed in the Appendix.
Immediate actions needed to control NZ's Campylobacter infection epidemic from chicken
As an island nation which produces all its own chicken, NZ is well placed to take immediate action to better manage this epidemic. The Ministry for Primary Industries (MPI), Food Standards Australia and New Zealand (FSANZ) and the poultry industry should assign a high priority to controlling the Campylobacter infection epidemic from fresh chicken meat based on its huge health and economic impact.
MPI should urgently review levels of Campylobacter on fresh poultry throughout the production and distribution system. The focus of monitoring is currently on testing chicken at the end of primary processing in plants across NZ, with results entered onto the National Microbiological Database (NMD). Introduction of this monitoring and associated actions was the key intervention that contributed to halving of human infections from this source during 2007.3
As described in the Appendix, contamination levels of Campylobacter in chicken reported on the NMD have dropped markedly since 2008 – a trend which is not mirrored in disease rates. Limited testing of fresh chicken meat at the point of sale has shown much higher levels of contamination than reported in the NMD at the same time.10 These findings suggest the need for measures to reduce contamination levels on fresh chicken at the point of sale, such as safer allowable limits, supported with systematic microbiological testing.
Consumers have a right to know about food safety risks. There are currently only minimal requirements for safety labelling of fresh chicken sold in NZ.11 FSANZ should act to correct this gap. Labelling could explain the likelihood and consequences of Campylobacter contamination on fresh poultry and key precautions to avoid illness (such as not washing the product, careful handling, and adequate cooking12). Information could also be provided to consumers to give an indication of the approximate level of contamination of specific brand and product lines, as has been used by the UK Food Standards Agency.13 However, measures to regulate food producers and their products are typically far more effective and cost-effective than educating consumers.14
Wider actions to reform food safety regulation in NZ
The persisting lack of progress in resolving the problem of foodborne Campylobacter infection in NZ suggests that responsibility for managing food safety should shift from MPI to an independent safety regulator. The last major advance in this area occurred under the leadership of the NZ Food Safety Authority (NZFSA), operating as a discrete government agency from 2002 to 2010 before ultimately being merged into MPI.
The NZ Government should consider a formal inquiry into this serious, long-term regulatory failure. The large Havelock North waterborne outbreak of Campylobacter infection resulted in an exhaustive inquiry and a complete reorganisation of the drinking water supply sector.15 16 That common source outbreak caused about 7,570 cases.17 By comparison, the ‘common source’ epidemic caused by contaminated chicken meat results in the equivalent of a Havelock North-sized outbreak every three months in NZ, or 80 such outbreaks since 2008.
What this Briefing adds
- NZ continues to suffer from an epidemic of Campylobacter infection caused by contaminated fresh chicken meat that has now persisted for more than 40 years.
- A strong regulatory response in 2007 reduced contamination levels in production plants and halved disease rates within 3-6 months, though most current cases (an estimated 77%) are still linked to chicken as the source.
- Over the subsequent 17 years from 2008 to 2024, contaminated chicken meat is estimated to have caused more than 600,000 cases of illness, over 9000 hospitalisations, at least 60 deaths, and economic costs of approximately $1.4 billion.
Implications for policy and practice
- NZ needs a comprehensive strategy to eliminate human infections from contaminated chicken meat.
- Industry and regulators need to upgrade the system of testing and quality assurance to reduce Campylobacter contamination levels of fresh poultry at the point of sale to consumers and potentially divert contaminated chicken through safer channels, notably as frozen and pre-cooked products.
- Regulators need to mandate labelling of fresh chicken meat to highlight the risk of infection, how to minimise it, and an indication of the level of contamination of each brand and product line.
- NZ needs to reinstate an independent regulator (equivalent to the NZFSA) with a strong mandate to restore the protection of citizens from contaminated food products.
- The NZ Food Safety Science & Research Centre (NZFSSRC) could consider supporting a programme of research to investigate key questions around how NZ can end this prolonged and serious epidemic.
Authors details
Prof Michael Baker Director, Public Health Communication Centre, and Department of Public Health, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington
Dr Leah Grout Southern California University of Health Sciences, Whittier, USA
Dr John Kerr, Science Lead, Public Health Communication Centre, and Department of Public Health, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington
Prof Nick Wilson Co director, Public Health Communication Centre, and Department of Public Health, Ōtākou Whakaihu Waka, Pōneke | University of Otago, Wellington
Acknowledgements
We acknowledge the large amount of work and collaboration between the poultry industry and MPI (and NZFSA before that) to establish and operate the NMD system.
We thank MPI for providing the NMD data and explaining the operation of some of the food safety measures being used by the poultry industry and regulators.
Jane Zhang for extraction and analysis of hospitalisation and mortality data.
Professor Martyn Kirk at The Australian National University for helpful peer review.
Appendix: Epidemiology and impact of Campylobacter infections from contaminated chicken meat in NZ
The methods used here to estimate the impact of Campylobacter infection from contaminated chicken meat in NZ have been previously published in a peer-reviewed journal article.1 This Briefing updates these estimates with more recent surveillance data up to the end of 2024. We have also refined key parameters based on reviewing those from other sources. Here we focus on the 17 years after regulations were successfully used to lower rates of infection from chicken meat in 2006-07.
Contribution of chicken meat as the source of this epidemic – The recent high-quality NZ source-assigned case-control study (SACNZ) found that 84% of human cases sampled in 2018-19 were infected with strains attributed to a poultry source of Campylobacter (a cattle source was next highest at 14%).9 This was a reasonably precise estimate (ie, we calculate the 95%CI interval from the published data to be 81.4% to 86.9%). The estimated proportion was 90% for those living in urban areas and 75% for rural cases.
The analysis for this Briefing excluded cases who had travelled in the preceding two weeks, who can be attributed to overseas sources. Surveillance data (Source: ESR Annual surveillance summaries) show that this proportion averaged 8% (7.8%) for the period 2008-23 (ranging from 0.3% in 2021 when overseas travel was minimal, to 14.2% in 2019). Consequently, an average of 92% of cases are estimated to be locally (NZ) acquired. Therefore, we estimate that 77% of cases can be attributed to chicken sources over this period (ie, 84% of 92%). The proportion in urban areas would be 83% (ie 90% of 92%) and in rural areas would be 69% (ie, 75% of 92%).
This SACNZ estimate of 84% is similar to that from a recent Australian source attribution study conducted in 2017-19 using similar methods. It concluded that “Our best fitting model estimated that chickens account for about 80% of campylobacteriosis.”18
It is important to note that the pathway from contaminated chicken meat to human infection will usually not be from eating chicken itself, unless it is undercooked. The SACNZ study found that there was no association between eating chicken and the risk of campylobacteriosis.9 Instead, the predominant pathway is likely be through cross-contamination from raw chicken, including through direct handling, contaminated surfaces in kitchens, and other foods prepared in the same settings. As this study states: “Poultry consumption per se was not identified as a significant risk factor. However specific risk factors related to poultry meat preparation and consumption did result in statistically significantly elevated odds ratios.” 9
Cases in the community – Campylobacteriosis is a notifiable condition for both diagnosing clinicians and laboratories in NZ. These data are collated by ESR at the national level. They recorded a total of 110,648 notified cases for the 17-year period 2008 to 2024. Using results from the source attribution study (77%) the contribution from chicken is estimated at a total of 85,199 diagnosed cases, an average of 5,012 per year over that 17-year period.
Only a small proportion of cases of symptomatic Campylobacter infection present to medical practitioners for diagnosis and treatment. And only some of the cases ultimately submit faecal specimens for laboratory testing. One high quality study conducted in the UK (the Infectious Intestinal Diseases Study, 201219) provides a credible multiplier of 9.3 for estimating the number of community cases for each notified case. Australia has used data from a survey of gastroenteritis and other sources to generate a multiplier linking reported numbers of Campylobacter infections to community incidence. Their estimate for Campylobacter infection is a multiplier of 10 (with a 95% credible interval of 7-22).20 The Havelock North outbreak of waterborne Campylobacter infection in 2016 found a case-ascertainment ratio of 7.3 (95%CI 6.8-8.0) based on 763 notified cases from 5540 gastroenteritis infections identified from survey data.17 Applying this more conservative NZ figure to notifications, suggests a total of 807,730 cases for the 17 years period 2008 to 2024, an average of 47,514 per annum. The contribution from chicken meat is estimated at a total of 621,952 symptomatic cases, an average of 36,585 per year, over that period.
Cases causing hospitalisations – People hospitalised with Campylobacter infection as the principal or additional diagnosis have been assigned a specific ICD discharge code since July 1995 (ICD-9 CM code 008.43 or ICD.10 ICD-10 AM code A04.5). These data provide probably the most consistent measure of Campylobacter infection trends over time because illness severity for hospital admission is likely to have been a reasonably consistent threshold over this period. It seems unlikely that poorer access to primary care for Campylobacter infection cases in some NZ settings will have done much to impact hospitalisation rates since it is rarely treated with antibiotics. That is, the mainstay of primary care treatment is supportive care such as recommending maintenance of hydration.
These hospitalisation data record a total of 11,120 discharges with a principle or additional diagnosis code for Campylobacter infection (after deducting repeat admissions within a month, which were approximately 5% of cases) for the 16-year period 2008 to 2023, an average of 695 cases per year. These cases were predominantly principal diagnoses (80%) throughout this period. For the entire 17-year period this would be an estimated 11,815 cases. The total contribution from chicken is estimated at 9,098 hospitalised cases, an average of 535 cases per year, over that 17-year period.
There has been a change in laboratory testing for enteric pathogens during this observation period that may have altered the sensitivity of methods for detecting Campylobacter. Both hospital and community laboratories have transitioned to nucleic acid amplification-based, culture independent diagnostic methods on various dates from 2015 to 2023.5 However, the trends for increasing hospitalisation rates and decreasing notification rates were established before this period.
Cases causing Guillain-Barré syndrome (GBS) – One of the most common serious sequelae of Campylobacter infection is GBS. This immune mediated condition damages the peripheral nervous system resulting in ascending weakness and sensory disturbance that typically evolves over several days. Most patients require hospitalisation and about one third need ventilatory support. The majority of patients recover but it is fatal for ~5% of patients in high-income countries and ~20% are still unable to walk at six months post-treatment.21
NZ research found that an estimated 25% of GBS cases are attributed to preceding Campylobacter infection.4 Hospital discharge data report a total of 1412 cases with a new principal or additional diagnosis of GBS over the 14-year period 2008-2021, an average of 101 cases a year or an estimated 1715 cases for the 17-year period. Based on 25% attributed to preceding Campylobacter infection, we estimate a total of 429 cases from this source or 25 cases per annum for the 17-year period from 2008 to 2024. The contribution from chicken is estimated at a total of 330 cases, an average of 19 cases per year over this period.
These GBS cases would have resulted in additional deaths attributable to contaminated chicken meat. The GBS admissions over the 14-year period 2008-2021 resulted in 65 deaths, which is a case fatality risk (CFR) of 4.6% (of the 1412 incident GBS discharges over that period). Applying this CFR to the estimated 330 cases, suggests 15 deaths can be attributed to preceding Campylobacter infection, with 12 attributable to contaminated chicken meat.
There are other common sequelae of Campylobacter infection, including reactive arthritis and inflammatory bowel disease that we have not estimated here, though some are included in the economic analysis.22
Cases causing death – Deaths from Campylobacter infection are generally poorly diagnosed and recorded. The death of Green Party Co-leader Rod Donald in 2005 from myocarditis secondary to Campylobacter infection, illustrates how this diagnosis can be missed initially.
Current reporting on the impact of Campylobacter infections lists very few deaths (eg, the national notifiable disease database (Episurv) is reported to have recorded a single death from Campylobacter infection in the 16 year period from 2008 to 20235). Consequently, we need to use other data sources to estimate the mortality burden from Campylobacter infections in NZ.
Hospital discharge data provide an indication of deaths in hospital. There were 60 reported deaths for patients with a discharge diagnosis of Campylobacter infection as the principal or additional diagnosis over the 14-year period 2008 to 2021, an average of 4.3 per year. National mortality data record 34 coded deaths as caused by Campylobacter infection as the underlying or contributing cause of death in the 11 years 2008-19, an average of 3.1 per year. Using the numbers in hospital discharge data would suggest a total of 73 deaths from Campylobacter infection during the 17 years 2008 to 2024, of which 56 or 3.3 per year could be attributable to poultry sources. Adding in an estimated 12 deaths from GBS from this source would increase the total to 68 or 4 per year.
That recorded mortality burden is likely to be a large underestimate. One reason is that many Campylobacter infection deaths are delayed. A registry-based linkage study in Sweden found that Campylobacter infections acquired domestically had an almost three-fold elevated risk of death in the first month post-infection (standardised mortality ratio of 2.9 (95% CI: 1.9–4.0)).23 In this study, risk gradually returned to baseline over the year following infection. In the Havelock North Campylobacter infection outbreak, hospitalised cases had a five-fold elevated risk of death within one year following discharge compared with non-hospitalised cases, though this risk was reduced after adjusting for age and comorbidities.24
The large waterborne outbreak of Campylobacter infection in Havelock North in 2016 resulted in a mortality risk of 72.2 per 100,000 cases (based on 4 deaths in 5,540 local residents with gastroenteritis identified from survey data,17 with two of these deaths in hospital24 ). Food safety scientists in Denmark estimate the case fatality risk (CFR) following Campylobacter infection at 69.5 per 100,000 (based on an estimated 41 deaths from 58,983 cases in 2019).25 Researchers at RIVM in the Netherlands have generated a similar estimate at 70.8 per 100,000 population (based on estimates of 201 deaths from 284,000 cases during 2019-23).26 These sources converge on a CFR of about 0.07% for Campylobacter infection.
Applying this risk estimate to NZ data of 807,687 cases, suggests a total of 583 deaths could be attributable to Campylobacter infection for the 17-year period 2008 to 2024, an average of 34 deaths per annum. The wide range of estimates for the mortality impact of NZ’s Campylobacter infection epidemic suggest that more investigation is needed, but these estimates give an indication of its potentially large scale. This impact represents the many lives which could be saved if this widespread exposure to Campylobacter could be substantially reduced.
Economic cost of Campylobacter from chicken meat – Campylobacter infection is the costliest foodborne disease in NZ, with estimated annual economic costs of NZ$134 million in 2006–2007.22 The rate halved after 2007, implying an annual cost of approximately $67 million at that time. Inflation adjusted to 2025, this would be $106 million per year. The total economic cost of Campylobacter infection for the 17 years since 2008 would therefore be approximately $1.8 billion dollars. Assuming 77% attribution to chicken would suggest economic costs of approximately $1.4 billion from contaminated chicken meat since 2008, an average of $82 million per year.
Other impacts – A further concern with widespread infection from contaminated chicken is that this pathway can contribute to the emergence and spread of antibiotic resistance from flocks to humans. This process was observed with the rapid rise of an antibiotic resistant clone of C. jejuni (resistant to tetracycline and fluoroquinolones) in locally-produced chicken and its spread to the human population in 2014.27
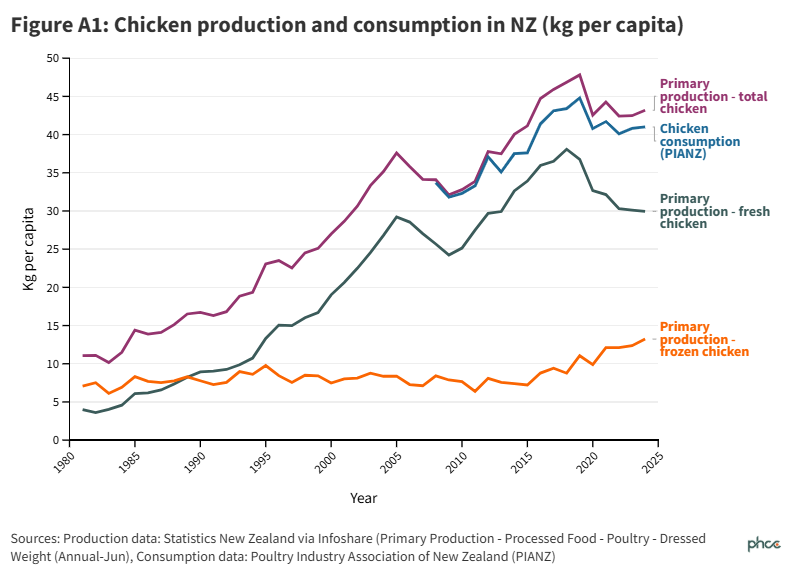
Poultry production and consumption – Figure A1 shows NZ data on chicken production and consumption (kg per person) by year. The production data from StatsNZ are for the 45-year period from 1980 to 2024. The consumption data (for 2008 to 2024) are reported by the Poultry Industry Association of NZ (PIANZ). The main observations are that:
- Overall chicken consumption per person rose approximately four-fold over that 45-year period.
- Most of that increase was driven by a rise in fresh chicken consumption which has now reached what appears to be a plateau of about 30 kg per person per year.
- Since 2008 there has been a small proportion of chicken exported, but otherwise NZ remains a largely self-contained system for chicken production and consumption.
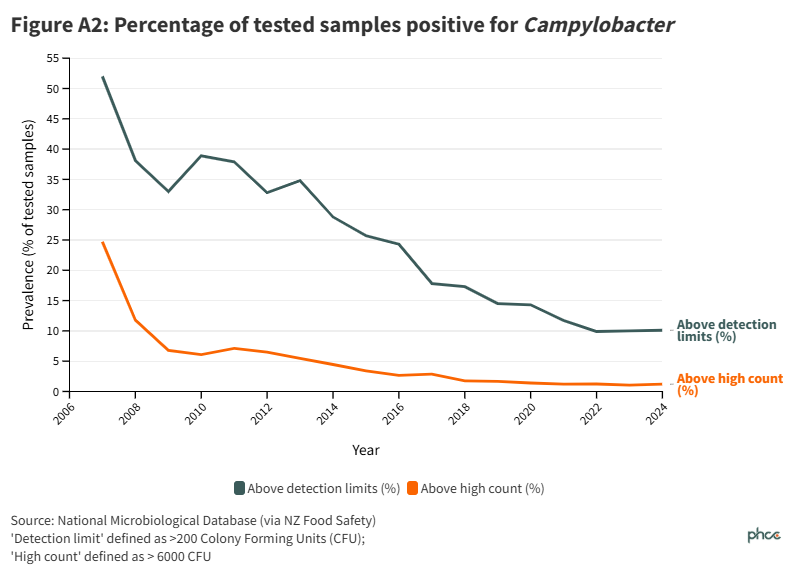
Contamination levels in chicken tested at processing plants – Figure A2 below shows the results of microbiological testing for Campylobacter on fresh chicken carcasses sampled at processing plants across NZ. These data are stored in the National Microbiological Database (NMD) managed by MPI. This systematic testing was introduced in mid-2007 as a key tool to monitor efforts to reduce contamination levels and for process control (regulatory action).3 A Campylobacter Performance Target (CPT) was first introduced for chicken meat in 2008.
The current testing methods are described in a technical manual (Ministry for Primary Industries, Animal Products Notice: National Microbiological Database Programme, February 2023.).
Data presented in Figure A2 are based on testing ~ 6,000 carcasses per annum from mid-2007 onwards. They show results for two thresholds of colony forming units (CFUs) detected per carcase sampled:
- Prevalence above detection limits (>200 / CFU per carcass rinsate, =2.3logCFU)
- Prevalence of high detections (>6000 CFU per carcass rinsate, =3.78logCFU )
It is important to note that prevalence below detection limits does not mean that the product is free of Campylobacter. Results cannot be used to estimate microbiological risk at other points in the supply chain.
Regulatory actions as described under the NMD Notice (Source: MPI, personal communication):
“Under the NMD programme, standard throughput premises (those that process more than 1 million birds in the season), are subject to the Campylobacter Performance Target (CPT). The CPT for meat chickens has two regulatory limits. These are:
- An enumeration target - where no more than 2 individual carcass rinse samples taken from one moving window may have Campylobacter counts greater than 6000 CFU per carcass (3.78 log10CFU/carcass); and
- A detection target that no more than 10 individual carcass samples taken from one moving window may have Campylobacter counts of 2.30 log10 CFU/carcass or greater
The moving window for the CPT is 3 successive processing weeks.
A CPT non-compliance occurs if either the enumeration or detection target is not met, in which case either an enumeration failure or detection failure is generated. A non-compliant moving window is recorded when a premises is recorded as having an enumeration failure, a detection failure or both.
The operator is required to undertake specific steps when a CPT non-compliance is generated.
- As soon as the operator is aware of a CPT non-compliance, they must notify their verifier within the next 24 hours.
- With each non-compliance review, corrective actions must be undertaken and any further actions planned to reach compliant status must be documented.”
“Over the last 5 years, MPI have not been required to take regulatory action. While there have been the rare occasions where the CPT is breached, the operator has been able to take effective corrective actions to avoid MPI intervention.” (Source: MPI, personal communication).
The results in Figure A2 show the large and rapid decline in high level detections that followed the regulatory intervention described here (introduction of NMD testing in mid-2007, and a CPT in mid-2008). This change was associated with a marked decline in Campylobacter infection rates in the community during 2007.
There was also a large, but slower, decline in positive detections (ie, chicken carcasses above the level of detection) from >50% in 2007 to <10% in 2020 (Figure A2).
In NZ, as in many comparable countries, the control of Campylobacter contamination during primary processing of chicken includes multiple physical and chemical decontamination steps. These methods are highly effective at reducing levels of contamination during this processing.28 Carcasses are sampled for the NMD at the start of secondary processing, which includes further processing steps (cutting up, trimming, skinning, deboning), prior to packing. Campylobacter concentrations in the final product after secondary processing were higher than at the end of primary processing in some plants, with a variety of mechanisms proposed for how this may occur.28
It is not clear how these NMD results relate to levels of Campylobacter in fresh chicken meat at the point of sale as there is little reported systematic testing at this level. One NZ study sampled fresh chicken (72 whole carcasses and 72 drumsticks) at the retail level in 2013-14. It found that 83.3% (60/72) of carcasses and 87.5% (63/72) of drumsticks were Campylobacter culture positive.10 The organisation “Consumer” tested a small sample of fresh supermarket chicken products in Dec 2016 and reported that 65.0% (26/40) were positive for Campylobacter. The prevalences detected in both these studies were much higher than those seen in the NMD at the time.
A potential reason for the contrast between these NMD results with the increasing rates of Campylobacter infection (based on hospitalisations), may be because of the problem of cross-contamination throughout the distribution system, and at the point of use by consumers as discussed earlier in this Appendix.
Ultimately, it may be necessary for a higher proportion of fresh chicken to be diverted down safer pathways, such as pre-cooked or frozen, which greatly reduces contamination levels.29
Uncertainties and further work that is needed – There are uncertainties inherent in all the data and estimates reported here. In general, these estimates are likely to be conservative. This particularly applies to estimated mortality related to Campylobacter infections, for the reasons described above. It would be valuable to conduct a more comprehensive analysis of the short- and long-term mortality effects of Campylobacter infection.
In some areas it would be important to update key research evidence, notably the economic analysis of the costs of Campylobacter infection in NZ that was reported in 2010.22 Such a study would need to include improved estimates of the mortality burden from Campylobacter infection.
It would also be important to repeat the source attribution study at some stage as it has a critical role in assigning the contribution that chicken sources make to all the estimates reported here. The high-quality SACNZ investigation used both a case-control study and whole genome sequencing of isolates to assign an attributable proportion to potential sources. It was conducted from March 2018 to March 2019, and reported in 2020, so findings are reasonably current.9
Important questions that remain unanswered by these data are around two large inconsistencies:
- The marked rise in Campylobacter hospitalisation rates during the 2008-23 period while notifications rates were falling. This inconsistency could be investigated with a detailed epidemiological study of these patient populations.
- The SACNZ study findings that 84% of human cases sampled in 2018-19 were infected with strains attributed to a poultry source of Campylobacter (adjusted to 77% after accounting for imported cases) when NMD data reported low contamination levels in carcasses tested at plants over that period. It would be useful to conduct systematic sampling of fresh chicken at the point of sale to measure the level of Campylobacter detected.
These are some of the questions that the New Zealand Food Safety Science & Research Centre (NZFSSRC) could consider investigating as part of a programme of research to identify how NZ can end this prolonged and serious foodborne epidemic.