There is no doubt that NZ needs to keep addressing ethnic inequalities in health as an important priority. Nevertheless, gender inequalities may also be worth some consideration given that NZ men have lower life expectancy than women by four years. This blog summarises key data and considers the major risk factors determining poorer male health. It then discusses if there is a plausible case for shifting more of the available health resources towards improving male health.
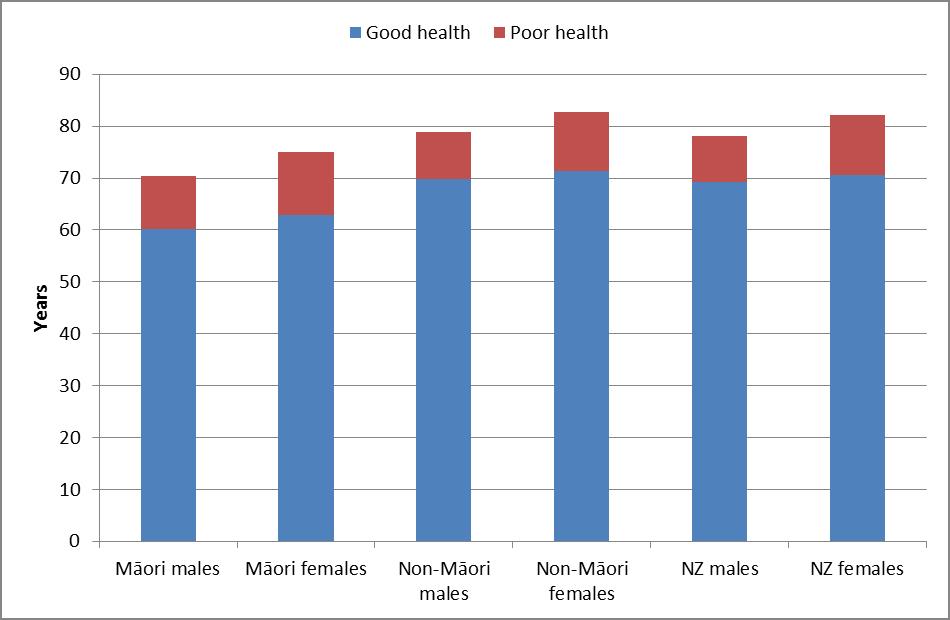
Figure: Years of life lived in good and poor health (based on data in: Ministry of Health 2013)
The key data has been produced by the Ministry of Health in a Major Report on health loss published last year. From the tabulated data the above graph has been prepared for this blog to show differences by gender and ethnic group. For males overall, the life expectancy difference (in 2006) was 4.0 years less than females. However, males lived an average of 1.4 years less in poor health (8.9 years vs 11.5 years). In other words males spend a slightly higher proportion of their shorter lives in good health, than do females (89% vs 86% of their lives).
What causes shorter NZ male life expectancy (relative to females)?
The Ministry Report detailed the higher injury burden among male youth (aged 15–24 years) and, to a lesser extent, among young adult males (25–44 years). In the next oldest age group (45–64 years) cardiovascular disorders are a key driver of the sex difference (eg, heart attacks). Among older adults, the most prominent sex difference is the greater burden of cancers in males (whereas in this age group females have more musculoskeletal disorders).
In terms of specific risk factors, the following were identified in the Ministry Report:
- “Alcohol-attributable injury burden is much greater in males than in females”,
- “About 70% of the burden of high dietary sodium falls on males” (this reflecting both higher salt intake and a higher total burden of coronary heart disease)
- “About 60% of the health loss from low vegetable and fruit intake is sustained by males”
- “About two-thirds of the health loss from high saturated fat intake is sustained by males” (and likewise for high cholesterol at 60%)
- “About 60% of the health loss from high blood pressure is sustained by males”
Do these differences in life expectancy matter much?
Probably “no” from a simplistic utilitarian perspective. Or only to a small extent given that the gap in healthy life is relatively small between the sexes. But perhaps a “yes” if the following are considered:
- There is a loss of human capital argument. Premature male deaths are often at young ages so society is particularly losing men from the workforce (eg, those young men dying on the roads or men in their 50s having fatal heart attacks).
- There is also perhaps an ethical argument. A major WHO Report has outlined criteria for determining if social inequity exists in health: “Three distinguishing features, when combined, turn mere variations or differences in health into a social inequity in health. They are “systematic, socially produced (and therefore modifiable) and unfair.” So while some gender differences will be substantially the result of non-modifiable biological differences (ie, oestrogen protects women from cardiovascular disease), it is likely that many differences in risk factors (eg, alcohol use, dietary patterns) are highly “socially produced” – hence suggesting some level around which gender differences in health are “inequitable”.
- More pragmatically, humans generally favour companionship – and so reducing the total number of “widow-years” (years lived as a widow or as a single post-partnership woman) is probably desirable at a societal level. This could be helped by differentially raising male life expectancy.
It would be good if these arguments were studied and voted on by a citizen jury composed of a random selection of NZers. Nevertheless, at first glance the above arguments seem to provide a reasonable case for doing relatively more to address poorer male life expectancy in NZ.
What could be easily done to increase male life expectancy in NZ?
Fortunately there are a range of possible population-level interventions that could be used. Because of the higher risk factor prevalence and disease rates among males, the same intervention across the population should have a relatively bigger impact on males than females. Examples of such interventions include:
- Intensify alcohol control – particularly cost-saving measures such as raising alcohol tax, restricting alcohol advertising, and reducing the availability of alcohol (eg, see this major review and this study for Australia and these two for Denmark (first study, second study).
- Reduce the maximum allowable salt levels in processed foods (something that may also be cost-saving, and if done at a slow rate will not even be noticed by consumers). Alternatively, a junk food tax could reduce dietary salt as well as intakes of saturated fat and sugar (but such taxes probably need to be carefully designed).
- Improve front-of-pack nutrition labels on processed foods – so that salt (sodium) and saturated fat levels are far more obvious eg, using a traffic light system – see a previous blog.
- Further improving the management of cardiovascular risk in those at high risk of heart attacks and strokes (and especially for Māori men for any targetted approaches so as to reduce both ethnic and gender inequalities together). There is a lot of activity in this area by the NZ health sector eg, “heart health checks” (which are quite probably cost-effective – but studies to show this definitively are needed). But more could be done. For example, patients on multiple cardiovascular medications could be switched to a single polypill – for which there is some evidence that NZ patients would favour. This could also save millions of dollars in the dispensing fees paid to pharmacists by the government.
The above strategies would be likely to also benefit female health, but probably not as much as male health (relatively speaking). Also of note is that some interventions could be cost-saving to society eg, particularly raising alcohol tax and regulating maximum salt levels in food. So perhaps some of these interventions could be described as being win/win/win – ie, a particular win for male health, an additional win for female health, and a collective win for reducing costs for the health sector.