Summary
New Zealand Health Survey (NZHS) data for 2023/2024 were released on 19 November. For the first time in a decade, the prevalence of daily smoking did not decline in Aotearoa, sitting at 6.9% (up from 6.8% in 2022/23).
Furthermore, unacceptable disparities in smoking prevalence persist for Māori, Pacific peoples, and people experiencing higher levels of deprivation.
These findings demonstrate that the government’s Smokefree Goal, commonly expressed as daily smoking prevalence falling below 5% for all population groups, is very unlikely to be achieved.
Unless there are dramatic falls in smoking prevalence among Māori, Pacific peoples, and people living in the most deprived areas, we will not reach a daily smoking prevalence of less than 5% for all population groups by 2025.
Smoking remains the leading cause of preventable disease and death in Aotearoa New Zealand, with large, persisting, and unacceptable inequities by ethnicity and neighbourhood deprivation.1
This briefing summarises key findings on smoking prevalence from the 2023/24 New Zealand Health Survey (NZHS). The NZHS is an annual nationally representative population survey that has run since 2011/12. It aims to sample around 14,000 adults aged 15 years and over every year (full details of the methods and the data presented in this article are available on the Ministry of Health website).
Overall smoking prevalence trends
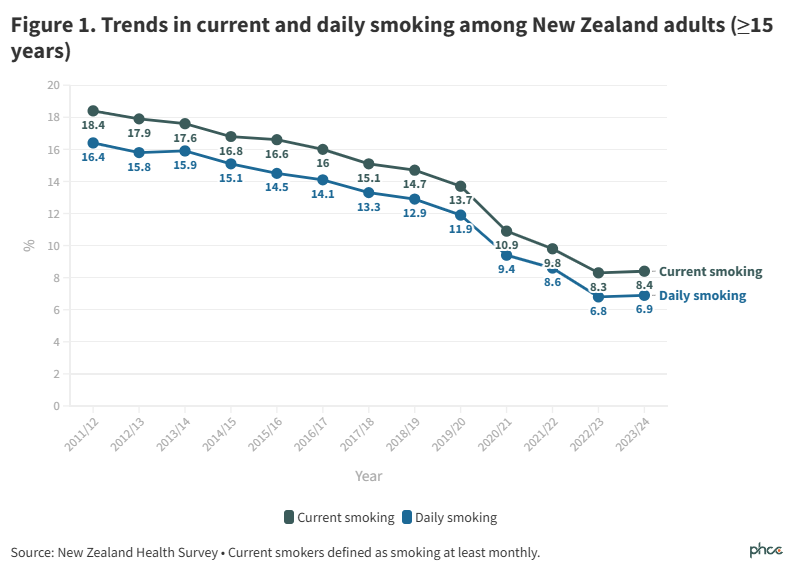
Daily smoking prevalence in 2023/24 was 6.9% (95% confidence interval (CI): 6.3-7.6%) and current smoking prevalence—smoking at least monthly—was 8.4% (95% CI: 7.7-9.1%) (Figure 1 and Appendix Table A1).
For the first time in a decade, daily and current smoking rates failed to decrease from the year prior (absolute increases of 0.1%). In contrast, daily smoking reduced by 2.5% from 2019/20 to 2020/21 and by 1.8% from 2021/22 to 2022/23.
The estimated number of people who smoked daily increased from 284,000 to 300,000 between 2022/23 and 2023/24.
Smoking prevalence and trends by ethnicity
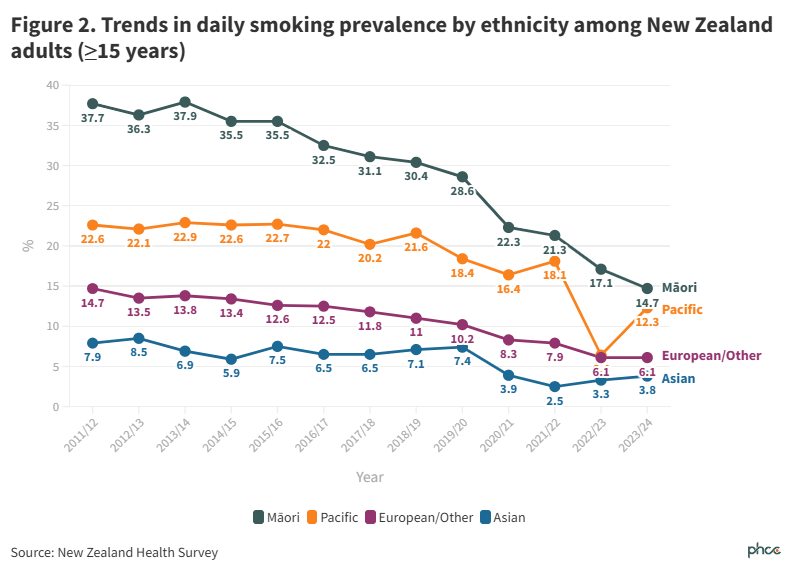
Substantial inequities in smoking by ethnicity persist, with daily smoking prevalence over twice as high for Māori and Pacific peoples compared to European/Other (Figure 2 and Table A1).
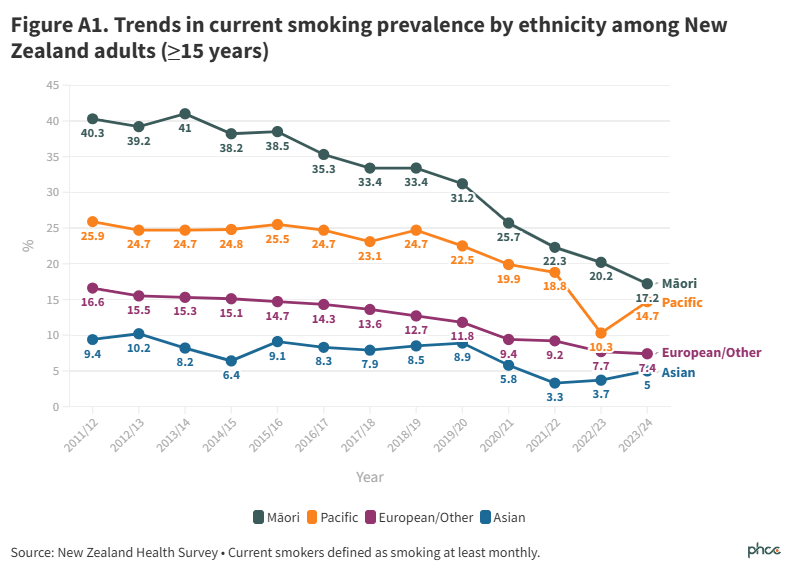
Daily smoking prevalence continued to trend downwards for Māori, from 17.1% (95% CI: 14.6-19.8) in 2022/23 to 14.7% (95% CI: 12.9-16.6) in 2023/24, an absolute (but not statistically significant) reduction of 2.4%. Current smoking prevalence among Māori also trended downwards from 20.2% (95% CI: 17.2-23.4) to 17.2% (95% CI: 15.2-19.4) (Appendix Figure A1).
Daily smoking prevalence for Pacific peoples reduced from 18.1% (95% CI: 12.1-25.4) in 2021/22 to 12.3% (95% CI: 9.2-16.0) in 2023/24, with current smoking reducing from 18.8% (95% CI: 12.7-26.3) to 14.7% (95% CI: 11.3-18.7) over the same period. The very low prevalences in 2022/23 may be due to a random fluctuation in sample characteristics resulting from small numbers in the Pacific sample.
On current trends, neither Māori nor Pacific peoples will have a daily smoking prevalence of 5% or less by 2025.
Smoking prevalence and trends by neighbourhood deprivation
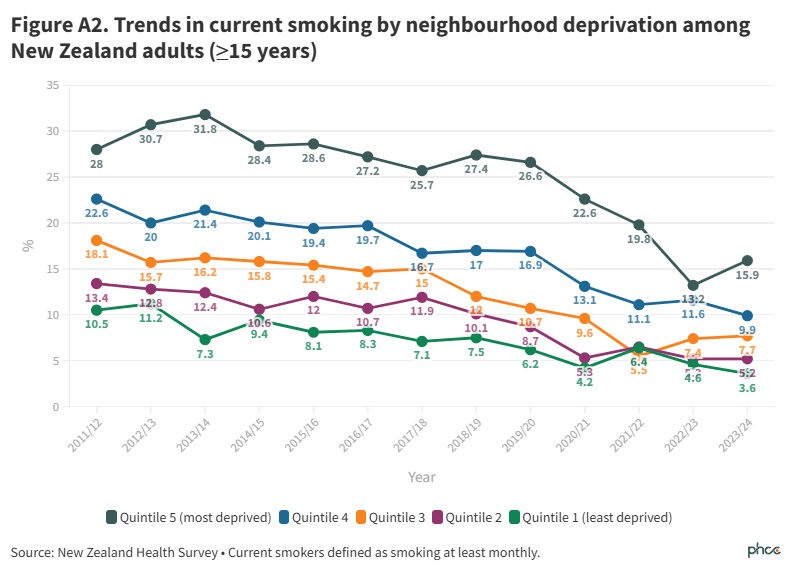
Inequities in daily smoking prevalence persist between the most and least deprived quintiles of neighbourhood deprivationNote, at 13.9% (95% CI: 12.1-15.8) in quintile 5 and 2.5% (95% CI: 1.4-4.0) in quintile 1 (Figure 3 and Table A1). Data on current smoking prevalence are presented in Appendix Figure A2.
Other than 2022/23, between 2017/18 and 2023/24 there was a four to five fold difference in daily smoking prevalence between people living in quintile 5 and quintile 1 .
Smoking prevalence and trends by age group and gender
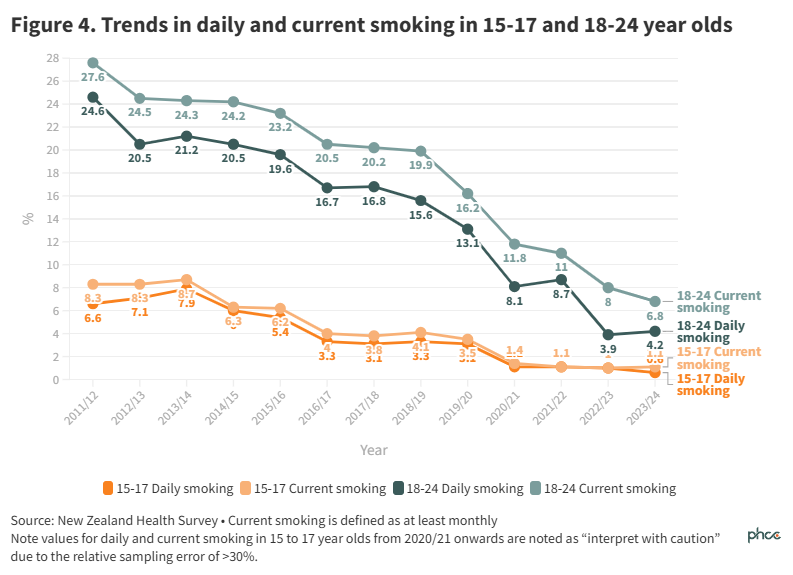
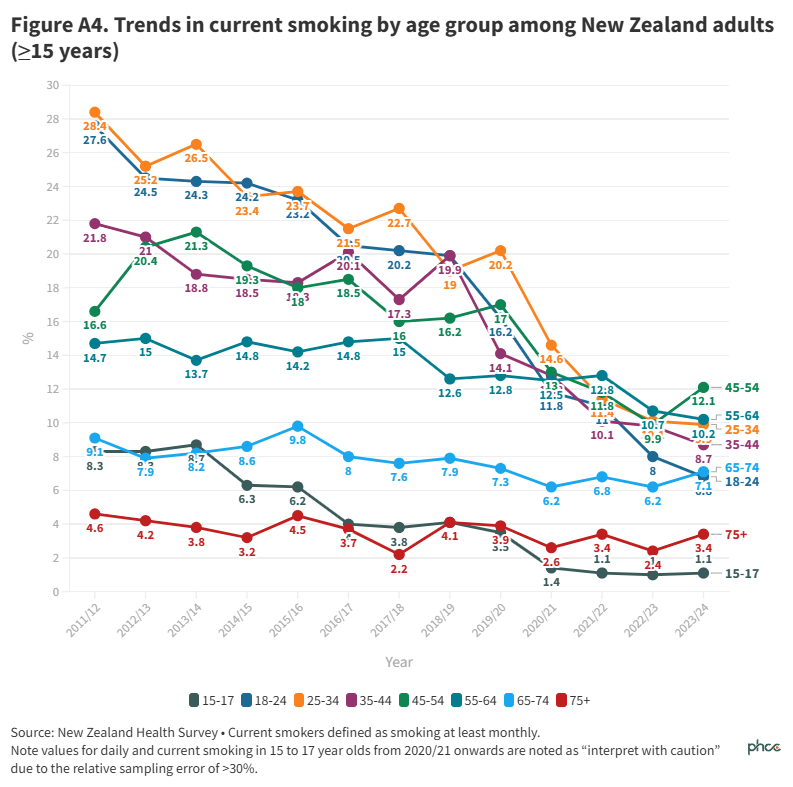
Daily smoking prevalence approximately plateaued in all age groups between 2022/23 and 2023/24, including among 15 to 17 and 18 to 24 year olds, where there had previously been long-standing declining trends (Figure 4 and Table 1A). Data for all age groups are presented in Appendix Figures A3 and A4.
Figure 5 and Table A1 show trends in daily and current smoking prevalence by gender and suggest that a gap in prevalence may be opening up between men and women. However, this possibility is based on a single survey, and further data is required to confirm if this is a trend.
Conclusions
For the first time in a decade, daily and current smoking rates failed to decrease from the year prior. Additionally, unacceptable inequities persist, particularly among Māori and Pacific peoples, and by neighbourhood deprivation. It is important to note differences in smoking prevalence reflect inequities faced by some population groups, including Māori and Pacific peoples, as well as structural factors, such as the concentration of tobacco product retailers in more deprived neighbourhoods.
The 2023/24 NZHS findings strongly suggest that the Smokefree Aotearoa 2025 Goal will not be achieved. Unless robust, effective, and equitable policies are implemented, we are highly unlikely to reach a daily smoking prevalence of less than 5% for all population groups by 2025. The time for the government to address the disproportionately light regulation of smoked tobacco products and their widespread availability is well overdue.2
What this Briefing adds
- In 2023/24, smoking prevalence did not decline compared to the previous year, with a daily smoking prevalence of 6.9%, representing an estimated 300,000 New Zealanders.
- Substantial inequities in smoking persist; daily smoking prevalences were substantially higher for Māori (14.7%), Pacific peoples (12.3%), and those daily living in them most deprived neighbourhoods (13.9%).
Implications for policy and practice
- Further public health measures are urgently needed to ensure the Smokefree Aotearoa Goal is achieved equitably and as quickly as possible.
Author details
Dr Janine Nip, Prof Richard Edwards, Prof Janet Hoek, Prof Andrew Waa
All authors are members of ASPIRE Aotearoa and the Department of Public Health, University of Otago, Wellington
Footnote: In the NZHS, neighbourhood deprivation refers to the New Zealand Index of Deprivation 2018 (NZDep2018), which measures the level of socioeconomic deprivation for each neighbourhood (Statistical Area 1) according to a combination of the following 2018 Census variables: household income, benefit receipt, household crowding, home ownership, employment status, qualifications, single parent families, living in home with dampness/mould and access to the internet.
Appendix
The New Zealand Health Survey also reports the prevalence of 'current smoking' defined as smoking monthly or more often. The figures below show trends in current smoking over time across demographic groups.
Table A1. Daily smoking values showing percentage with 95% confidence intervals in brackets
| | 2020/21 | 2021/22 | 2022/23 |
| Total | 8.6 ( 7.7 - 9.7 ) | 6.8 ( 6.1 - 7.5 ) | 6.9 ( 6.3 - 7.6 ) |
| | | | |
| Ethnicity | | | |
| Māori | 21.3 ( 17.7 - 25.3 ) | 17.1 ( 14.6 - 19.8 ) | 14.7 ( 12.9 - 16.6 ) |
| Pacific | 18.1 ( 12.1 - 25.4 ) | 6.4 ( 4.1 - 9.3 ) | 12.3 ( 9.2 - 16.0 ) |
| Asian | 2.5 ( 1.3 - 4.5 ) | 3.3 ( 1.8 - 5.6 ) | 3.8 ( 2.3 - 5.8 ) |
| European/Other | 7.9 ( 6.7 - 9.1 ) | 6.1 ( 5.3 - 7.0 ) | 6.1 ( 5.4 - 6.7 ) |
| | | | |
| Neighbourhood deprivation | | | |
| Quintile 1 (least deprived) | 4.6 ( 2.7 - 7.3 ) | 3.1 ( 1.9 - 4.7 ) | 2.5 ( 1.4 - 4.0 ) |
| Quintile 2 | 5 ( 3.1 - 7.8 ) | 4.3 ( 2.8 - 6.3 ) | 4.3 ( 3.3 - 5.7 ) |
| Quintile 3 | 5 ( 3.4 - 7.0 ) | 6.1 ( 4.6 - 7.9 ) | 6.1 ( 4.8 - 7.5 ) |
| Quintile 4 | 9.9 ( 7.8 - 12.3 ) | 9.8 ( 7.7 - 12.2 ) | 8.3 ( 6.9 - 9.9 ) |
| Quintile 5 (most deprived) | 19.1 ( 16.2 - 22.3 ) | 10.7 ( 8.6 - 13.2 ) | 13.9 ( 12.1 - 15.8 ) |
| | | | |
| Age | | | |
| 15-24 | 6.5 ( 4.0 - 9.9 ) | 3 ( 1.8 - 4.6 ) | 3 ( 2.0 - 4.3 ) |
| 25-34 | 9.8 ( 7.4 - 12.7 ) | 7.9 ( 6.0 - 10.2 ) | 7.8 ( 6.3 - 9.5 ) |
| 35-44 | 9 ( 6.4 - 12.2 ) | 7.8 ( 6.0 - 9.9 ) | 6.9 ( 5.6 - 8.3 ) |
| 45-54 | 10.7 ( 8.0 - 13.8 ) | 8.5 ( 6.5 - 10.8 ) | 10.8 ( 8.7 - 13.3 ) |
| 55-64 | 11.4 ( 9.0 - 14.1 ) | 9.7 ( 7.5 - 12.2 ) | 9 ( 7.4 - 10.9 ) |
| 65-74 | 6.8 ( 4.8 - 9.3 ) | 5.9 ( 4.2 - 7.9 ) | 6.2 ( 4.7 - 8.1 ) |
| 75+ | 3.2 ( 1.9 - 5.2 ) | 2.4 ( 1.5 - 3.7 ) | 3.1 ( 2.2 - 4.2 ) |
Note: As the survey draws on sample of people and not the whole population, the confidence intervals in this report provide an indication of the lower and upper limits of the range of values.