Summary
Aotearoa New Zealand (NZ) risks a large measles epidemic. Child immunisation coverage at two years of age has been falling and is now 83% overall, and 69% for Māori children. This is far below the 95% target level needed to maintain measles elimination. This decline adds to historical gaps in immunisation coverage, particularly for adolescents and young adults. Inbound international travel has returned to near pre-pandemic levels. With global measles increasing, more infectious cases will enter NZ.
To prevent a measles epidemic urgent steps are needed to catch up those who have missed out on vaccination, alongside continuing work to increase routine childhood coverage, particularly for Māori, Pacific Peoples, and deprived communities. NZ needs to immediately decrease the risk of importing cases from countries with measles transmission and exporting infections to Pacific Islands. We also need to strengthen epidemic response capacity across the public health, healthcare, and educational sectors.
Aotearoa New Zealand (NZ) is vulnerable to a national measles epidemic. The World Health Organization (WHO) Regional Verification Commission (RVC) for Measles and Rubella Elimination has concluded that “… New Zealand is at risk of a large outbreak and losing its elimination status, unless immunity gaps are rapidly closed”.1 Local assessments agree.2 3
This Briefing summarises the reasons why NZ is vulnerable to a measles epidemic and the urgent actions needed to reduce the risk and consequences of such an event, in addition to current efforts to increase childhood immunisation coverage.
A severe measles epidemic is likely
In the pre-vaccine era, measles was a near universal infection for children, and a leading cause of child deaths. Measles vaccine was added to the routine childhood immunisation schedule in 1969. Since 2019, two doses of measles, mumps, rubella (MMR) vaccine are scheduled, at 12 and 15 months. The history of measles and vaccination is described in the Immunisation Handbook 4 and in the appendix.
There are multiple reasons for concern:
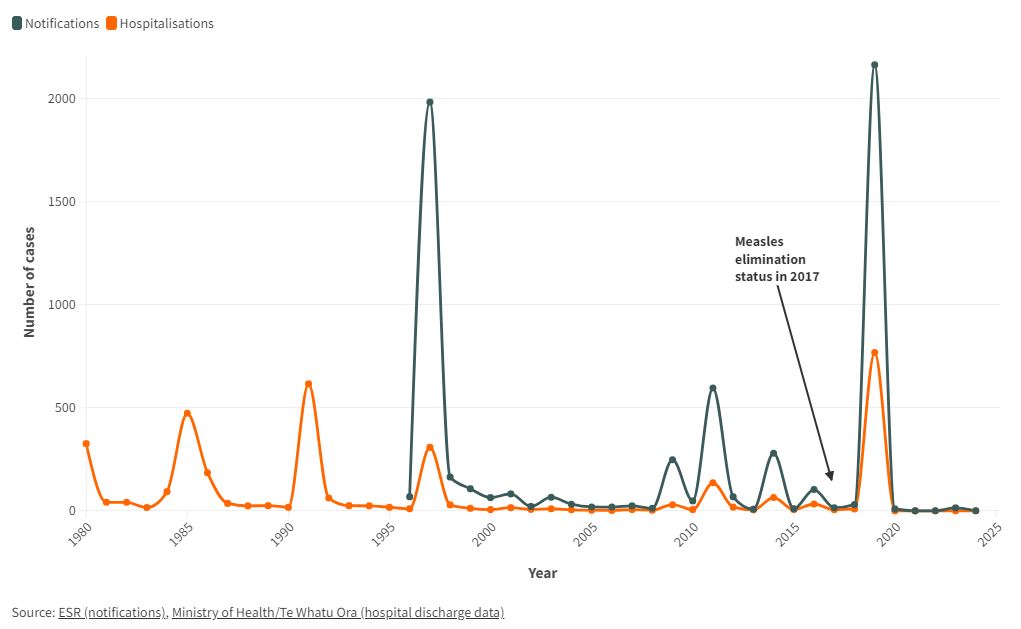
- Measles is a serious illness for people of any age, including pregnant women. In the last national outbreak in 2019, 35% (775/2213) of cases were hospitalised for treatment of complications.4
Figure 1. Measles annual incidence of notified and hospitalised cases, 1980 to 2023. Source: ESR (notifications) and Ministry of Health/Te Whatu Ora (hospital discharge data)
- Measles is a devastating illness in low- and middle-income countries. The NZ outbreak in 2019 spread to Samoa where it caused 5707 cases and 83 measles-related deaths.5
- Measles is one of the most infectious diseases known, with one case typically infecting 12-18 others in a non-immune population.6 Preventing outbreaks and achieving elimination requires 95% coverage with two doses of measles-containing vaccine in each birth cohort with no major population groups missing out.7
- Historically, NZ had low immunisation coverage in the childhood programme, with significant equity gaps by ethnicity, socioeconomic status, and geography. In 1991 less than 60% of NZ children were fully immunised by two years of age, with only 42% of Māori and 45% of Pacific children immunised.8 While coverage in the childhood programme has improved since that time, along with a range of catch up measures, the legacy of low coverage has left concerning gaps across most cohorts born since 1969 (those now up to 55 years of age).8
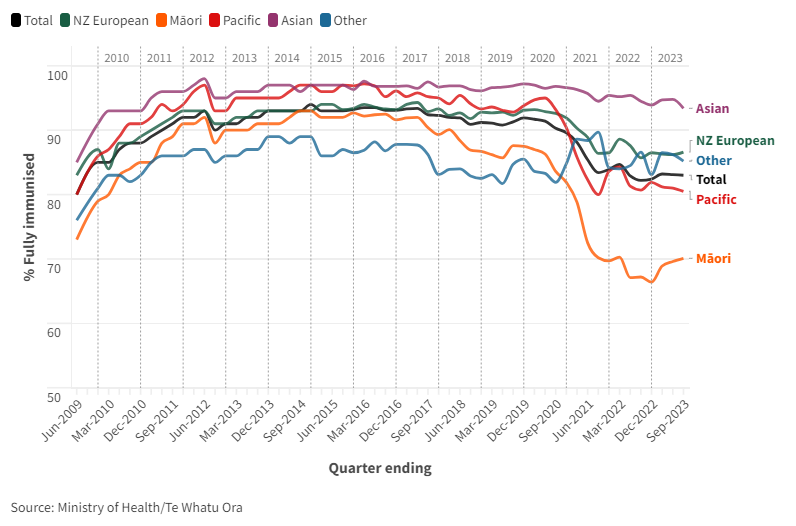
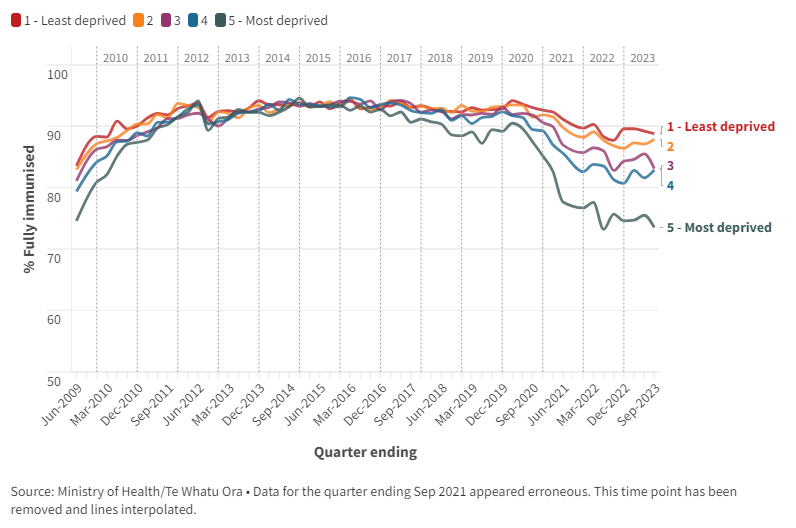
- The routine childhood vaccination programme is not achieving sufficient coverage.3 Coverage peaked in 2013-17, but has fallen since then and is currently at its lowest level since 2009 (Figure 2). In 2023 coverage at two years was 83% overall, but only 69% for Māori, 81% for Pacific children, and 75% for children in the most deprived communities, (NZDep 9-10) (Figures 2 and 3).
Figure 2. Immunisation coverage at 2 years of age, by ethnic group, by quarter 2010 to 2023.
Figure 3. Immunisation coverage at 2 years of age, by household deprivation, by quarter 2010 to 2023.
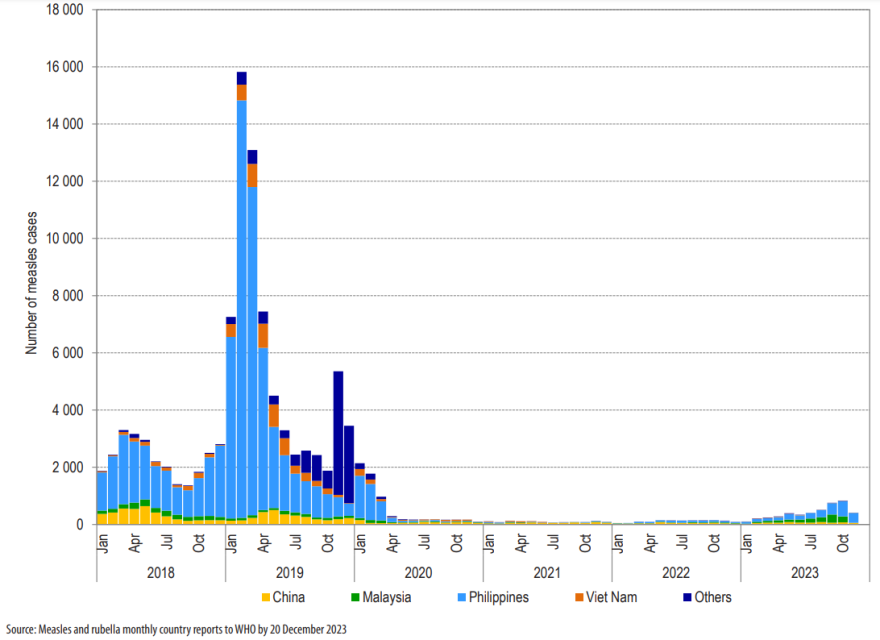
- The risk of measles importation is increasing as global coverage also declined during the pandemic.9 Measles rates are rising internationally, including in the UK, Europe, US, and several countries in our Western Pacific region, notably the Philippines, Malaysia and China (Figure 4).10
Figure 4. Measles incidence in the World Health Organization (WHO) Western Pacific Region by country and month, 2018-2023. Source: WHO Regional Office for the Western Pacific.10
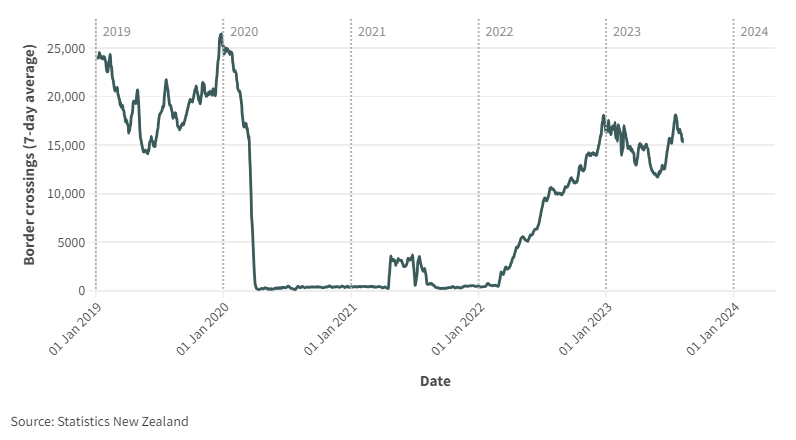
- In addition, travel into NZ has almost returned to pre-pandemic levels, with around 20,000 people entering each day in January 2024 (Figure 5) so there are more infected people arriving in NZ.
Figure 5. Arrivals to NZ by day, rolling seven-day average, January 2019 to January 2024.
This situation means that NZ is at high risk of a national measles epidemic1 which would have many negative health, social, and economic effects:
- Multiple measles cases, hospitalisations, and potentially some deaths.
- Long-term effects on the health of survivors, including from encephalitis , pneumonia, and immune depletion affecting immune response to other infections.11
- Likelihood of exporting measles to Pacific Islands and potentially other countries with devastating effects.5
- Disruption caused by a national epidemic and control measures, including closure of schools and early childhood education (ECE) centres during outbreak periods.
- Diversion of public health resource to support control measures, including case isolation, contact tracing and quarantine measures.
Actions to prevent and mitigate a measles epidemic
Urgent action in the absence of widespread disease can be a difficult sell. But responding to an outbreak will cost a lot more than preventing it. Urgent action is needed in four broad areas:
1. Reduce the risk of importing measles – All travellers to NZ should be routinely asked to check their measles vaccine status and that of their children when they book their travel, bring documentation of their status with them, and vaccinate if susceptible. New Zealanders travelling overseas should be given similar advice. A range of other measures are needed, including steps to reduce transmission to Pacific Islands (see appendix).
2. Catch-up immunisation for children and young adults – There is a critical need to fill immunity gaps before measles arrives. This means catching up those in ECE centres, schools, and young adults and new parents who have missed out. Equity is critical, so there is a particular need to close immunity gaps for Māori and Pacific children (Figure 2) and those living in relative deprivation (Figure 3). Multiple strategies need to be considered including: supporting Māori-led immunisation programmes that engage effectively with communities; responding to misinformation/disinformation relating to vaccination; improving use of the Aoteoroa Immunisation Register (AIR) to track under-vaccination and support vaccine delivery; school-based delivery; and considering incentives for providers and families.12-14
3. Continue work to raise coverage through the routine childhood immunisation programme – An Immunisation Taskforce produced a set of recommendations to lift childhood coverage that are largely focussed on the routine programme but include some catch-up measures.3 Health Minister Dr Shane Reti has announced a $50 million investment in measures to raise vaccination rates with a priority focus for Māori.
4. Prepare to manage outbreaks when they occur – The Ministry of Health commissioned an independent review of the response to the 2019 measles epidemic, submitted in July 2020.15 It identified multiple areas for enhancement. These recommendations need to be revisited and acted on if not already completed, along with other measures (see Appendix).
What this Briefing adds
- Measles (MMR) vaccine coverage is too low to maintain elimination and NZ will face increasing numbers of imported cases until global control improves.
- There is particularly low coverage for Māori and Pacific children and those in deprived communities that are likely to be more vulnerable to rapid spread of measles.
- It is only a matter of time before an import sparks an outbreak. The numbers of susceptibles could make this the largest epidemic since the 1990s with thousands of cases, hospitalisations, chronic illness, and potentially deaths. A NZ epidemic could also spread to Pacific countries.
Implications for policy and practice
- NZ needs to urgently reduce the risk of imported measles by encouraging all those travelling to NZ, and all New Zealanders travelling overseas, to check their measles immunity and get vaccinated if susceptible or uncertain.
- It is also urgent to rapidly address immunity gaps, with the priority in ECE centres, schools, and other institutions where many people mix. For disease control and equity, we need to prioritise immunisation strategies to reach Māori, Pacific, and the most deprived children.
- The Aotearoa Immunisation Register (AIR) should be more widely used to track and offer vaccination to all born since 2005 without documentation of two MMR doses.
- NZ needs to prepare for measles outbreaks across the country, including procedures to ensure safe management of cases presenting in healthcare and educational settings, and comprehensive documentation and follow up of the measles immunity status of children attending ECE centres and schools.
Author details
Prof Michael Baker, Department of Public Health, University of Otago Wellington, and Public Health Communication Centre
Prof Nikki Turner, Department of General Practice and Primary Care, University of Auckland, and Medical Director of the Immunisation Advisory Centre
Dr Mamaeroa David, GP, McLaren Park Medical Centre
Assoc Prof Amanda Kvalsvig, Department of Public Health, University of Otago Wellington
Dr Oz Mansoor, Medical Officer of Health, Tairāwhiti
Prof Nick Wilson, Department of Public Health, University of Otago Wellington, and Public Health Communication Centre
Appendix: Additional information on measles epidemiology, prevention, and control in NZ
Measures to reduce the risk of importing measles into NZ
- All travellers to NZ should be routinely asked to check the measles vaccine status of those in their party (born after 1969) when they book their travel. Vaccination would be advised as documented immunity would mean they would avoid the need for quarantine if they become a close contact of a case while in NZ during a measles epidemic.
- New Zealanders travelling overseas should be given similar advice to protect their own health, and avoid bringing measles back into NZ.
- Measles vaccination and enrolment in AIR should be added as a requirement for all migrants to NZ, as we know many have missed vaccination in their countries of origin.16
- There is potential to evaluate (in the NZ context), the utility of testing for measles virus in the wastewater of arriving aircraft, as has been done to detect imported Covid-19 (SARS-CoV-2 virus).17 18 Such testing could inform risk assessment, case identification (when positive), and could be a trigger for media alerts that inform the public of the ongoing risk and the need for vaccination. There is even a case for NZ to be part of a “global aircraft-based wastewater genomic surveillance network” to warn about future pandemics.19
Measures to better manage measles outbreaks and epidemic spread when these occur
- The Ministry of Health commissioned an independent review of the response to the 2019 measles epidemic, submitted in July 2020.15 It identified multiple areas for enhancement including: improving immunization coverage and service delivery; improving outbreak management; strengthening governance and oversight; making optimal use of digital technologies; and prioritising equity considerations for Māori and Pacific populations in the management of immunisation and outbreaks. It will be important to review progress with implementing these recommendations.
- The National Public Health Service of Te Whatu Ora will need to review capacity for rapidly managing large numbers of measles cases and their contacts.20 The Communicable Diseases Control Manual21 specifies that cases should be isolated for at least four days after the appearance of the rash. And unvaccinated (or partially vaccinated) contacts should be offered MMR vaccine and can be quarantined for up to 14 days post exposure. In the early stages of an outbreak, rapid whole genome sequencing (WGS) has potential to help in tracking the spread of measles infections.22
- Schools and ECE centres are required to manage workplace risks, including any potential or actual outbreaks of communicable diseases. This obligation includes asking students, children and staff showing signs of communicable diseases to stay at home. These requirements would extend to contacts of measles cases – as noted above. There are known to be immunisation gaps in key occupational groups who work with children such as ECE centre staff.23 The likelihood of a national measles epidemic should be an incentive to encourage staff vaccination.
- All schools and ECE centres need to document the measles vaccination status of all attendees.4 The Health (Immunisation) Regulations 1995 require parents/guardians of children to show their child’s immunisation certificate when these children start at an ECE centre or primary school. Doing this would make it easier to manage quarantine arrangements (eg, online learning) for non-vaccinated students who have had contact with measles cases. Post-exposure vaccination (or, if indicated, intravenous immunoglobulin) can also be offered.
- The possibility of an outbreak in an emergency department (ED) is a significant risk as this is where undiagnosed or newly-diagnosed cases are likely to present. Preparation could include: education to support early case recognition; development of a multidisciplinary, pre-incident response plan including a strategy for patient flow that avoids shared air; short laboratory turnaround time for diagnostic testing; and up-to-date record-keeping to identify healthcare workers who may need post-exposure prophylaxis.24 High-quality (respirator) masks should be available for both infected persons and their contacts, which includes any person in the same indoor space. Te Whatu Ora guidelines for measles in healthcare settings appropriately recommend respirators for staff but they still recommend surgical masks for suspected cases, which would not be effective against this highly transmissible virus.
- Measles is spread through the air and transmission is enhanced in crowded settings where ventilation is poor. Alongside vaccination, improved indoor air quality in schools can help to reduce transmission of a number of common viruses, including measles.25 26 Similarly, high ventilation standards (including use of airborne infection isolation rooms [AIIRs]) are needed to prevent nosocomial (hospital-acquired) transmission of measles. Nosocomial measles outbreaks typically have higher severity than community outbreaks for several reasons.27 They can lead to infection of both healthcare workers and patients.28
- The high risk of a national measles epidemic is a further justification for implementing an integrated respiratory infectious disease surveillance and control strategy, that also aims to reduce the public health impact of Covid-19, influenza, RSV and other respiratory infections.29
- Because of years of successful elimination in NZ, primary care practitioners, teachers, and parents may be unfamiliar with measles, so an awareness campaign may be needed to facilitate early recognition of cases in the community. There are on-line resources which can assist, eg KidsHealth https://www.kidshealth.org.nz/measles
- NZ should review processes for preventing spread of measles to Pacific countries if an outbreak occurs. These processes could include exit screening, and potentially requirements for evidence of measles vaccination for those travelling to Pacific countries during an outbreak or epidemic in NZ.
Notes on the history of measles and vaccination in NZ
The perception of measles has changed from the pre-vaccine era when it was a near universal experience for children. Now that we are aiming to be measles-free a single case is considered an outbreak.
Measles vaccine was added to the NZ immunisation schedule in 1969. Until the 1980s, coverage was too low to change the pre-vaccine cycle of 2-3 yearly epidemics. And until 1992 there was only a single dose in the schedule. Two doses of vaccine are needed to address the ~10% who fail to be protected by the first dose (otherwise even at 100% coverage at one dose we would not reach the immunity threshold of just under 95% (1 -1/ R0).
The inter-epidemic period increased to 5-6 years following the 1978 ‘measles eradication programme’ with epidemics in 1980, 1985, 1991 and 1997.
In 1992, a second dose of MMR vaccine (that had replaced measles vaccine in 1990) was added to the schedule at age 11 years. The 1997 epidemic showed that the second MMR dose was too late. So, MMR2 was moved to age 4 years and in 2019 to age 15 months. A history of measles and vaccines is available in the Immunisation Handbook.4
The first large outbreak since 1997 was in 2019, two years after WHO declared measles eliminated in NZ in 2017. WHO certification was based on the absence of endemic virus transmission for a continuous period of ≥36 months in the presence of a high-quality surveillance system.4
Immunity gaps in young adults and communities with low coverage allowed measles to circulate for nearly a year. But high coverage in the primary school population limited community spread (cohorts born from 2011-2016 having close to 95% immunity). Transmission stopped in just under 12 months, so we retained our elimination status.
Paradoxically, immunisation can lead to higher levels of adult susceptibility. For those born before the 1980s, the continuing 2-3 inter-epidemic cycle means that nearly all would have been infected by the time they were adults. As coverage rises, it increases the chance of not being exposed during childhood. This population effect (‘herd immunity’ or indirect protection) increases the chance of reaching adulthood still susceptible to measles.
In 1991 less than 60% of NZ children were fully immunised by two years of age, with only 42% of Māori and 45% of Pacific children immunised.8 MMR1 coverage was 82%, a second dose was not added until 1992.
From the 1980s to mid-1990s when coverage started improving, measles vaccine coverage hovered between around 75 to 80%. Since 1997, there has been limited nation-wide exposure to measles. The last national measles campaign was also delivered in that year, targeting children aged 2-10 years, but with variable and poorly documented coverage. These cohorts, now aged 27 to 44 years will have a lower proportion susceptible than those while coverage was improving but not close to 95% target with two doses.
Coverage improvements accelerated with the National Immunisation Register which contains all registered immunisation enrolments and events for children born since 2005.30
Those born between 2011 and 2016 (approximately) had close to the 95% target with two doses. These children, aged 3 to 8 years created an ‘immunity wall’ that limited the extent of the 2019 outbreak, fuelled by other gaps.
In 1996, we predicted a measles epidemic based on the calculated number of susceptible children aged under 10 years that had triggered the three previous epidemics.31 It turned out that by 1996 we had breached the lower threshold of 130,000 children aged under 11 years (just over two birth cohorts). The epidemic started in early 1997, just before a planned preventive campaign.32
Childhood immunisation coverage fell after 2017 and is now at its lowest level since 2009 (Figure 2). Overall coverage at two years is now 83% compared to 91% in 2019 which was our last national epidemic. Even more concerning is the much lower coverage for Māori children (69% at two years) Pacific children (81%) and those living in the most deprived communities (75% in NZDep9-10)(Figures 2 and 3).
These coverage levels are markedly lower than comparable countries such as Australia, where the national coverage rate was 91% for two year olds at September 2023. Coverage was only slightly lower for Aboriginal and Torres Strait Islander children at 89%.
Measles is not currently endemic in NZ, so outbreaks can only be initiated when infected cases arrive as travellers from overseas.33 It has a relatively long incubation period (median of 14 days, range 7-21 days, from exposure to onset of characteristic rash34) so it is easy for travellers who are exposed overseas to appear well when entering NZ. Because people are infectious for four days before onset of the rash34 they can easily infect other people on the same flight.336
The Covid-19 pandemic response37 temporarily helped to sustain measles elimination by preventing introduction of cases (along with also halting influenza and other respiratory infections38) until the borders were re-opened in 2022. It was not until 2023 that we started seeing imported measles – with three events, each of which led to large public health responses to identify and isolate multiple close contacts potentially exposed to a case in their infectious period.