Summary
New Zealand Health Survey (NZHS) data for 2024/2025 were released on 19 November 2025. Daily vaping prevalence was 11.7% in 2024/25 among adults aged ≥15 years, which is similar to the prevalence in 2023/24 (11.1%), but higher than in 2019/20 (3.5%). Over half a million people were estimated to be vaping daily in 2024/25.
Daily vaping was much higher among younger age groups, Māori, Pacific peoples, and people experiencing higher levels of neighbourhood deprivation.
The impact of recent (June 2025) vaping regulations, including measures aimed at ending sales of disposable vapes, are not captured in the 2024/25 NZHS data. Analysis of subsequent surveys is needed to determine whether the 2025 regulations reduce daily vaping — especially among groups with the highest vaping prevalence — or whether stronger regulatory action and enforcement might be needed.
High levels of vaping among adolescents and young people have created great concern among parents, communities and schools, public health practitioners and researchers, and health workers. In response, regulatory changes implemented between September 2023 and June 2025 aimed to reduce uptake of vaping among adolescents and young people. New measures include restrictions on: specialist vape store locations, visibility of vaping products in retail settings, and youth-appealing packaging and flavour names. New nicotine concentration limits in e-liquids have been introduced and disposable vapes may no longer be sold. The changes are summarised in Appendix 1.
This Briefing summarises key updates on vaping prevalence from the 2024/25 New Zealand Health Survey (NZHS). Appendix 2 provides methodological information about the survey. A recent accompanying Briefing1 provides a summary of NZHS findings on smoking prevalence.
Key findings
Population trends
Adult daily vaping increased significantly from 3.5% (95% confidence interval [CI]: 3.0-4.0) (See Appendix 2, endnote 1) in 2019/20 to 11.1% (95%CI: 10.4-11.9) in 2023/24. It was similar in 2024/25 at 11.7% (95%CI: 10.7-12.8) (Figure 1, Appendix 3 Table A1). An estimated 509,000 people were vaping daily in 2024/25. Prevalence of ‘at least monthly’ and ‘ever tried’ vaping did not change significantly between 2023/24 and 2024/25. In 2024/25, most people (85%) who vaped at least monthly were daily users.
Figure 2 shows that around 17% of adults smoked or vaped daily (or both) in 2023/24 and 2024/25. The figure shows that the decrease in daily smoking since 2017/18 has been accompanied by a larger increase in daily vaping prevalence, with total daily nicotine use increasing from 14.7% to 17.1%.
Vaping by age group
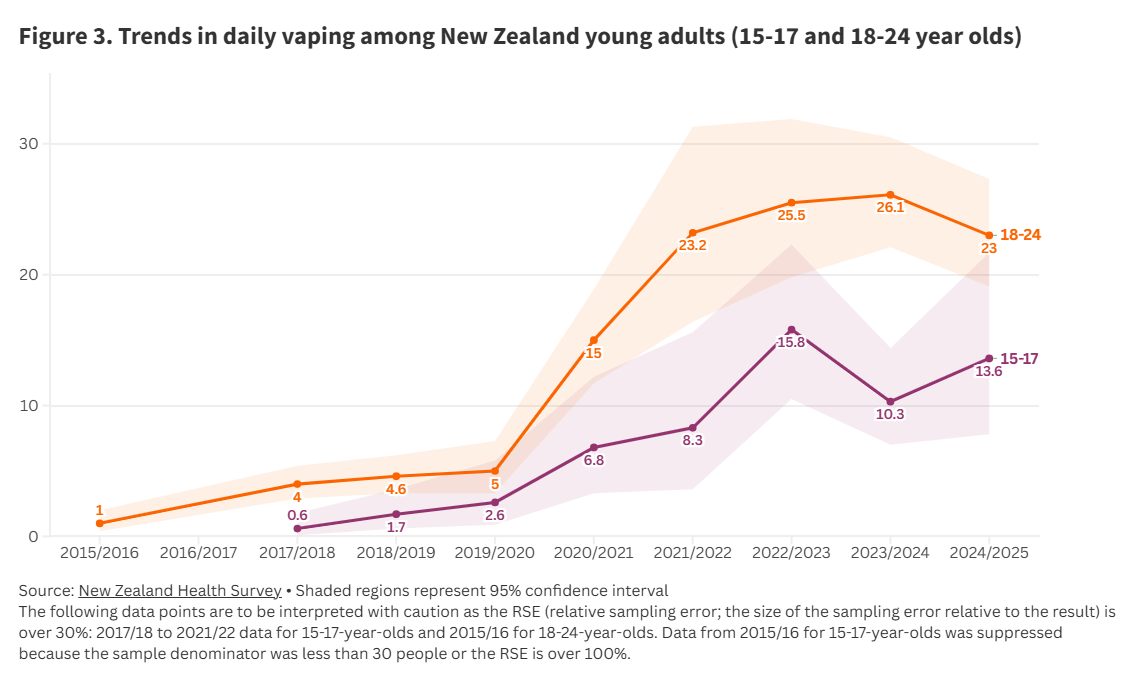
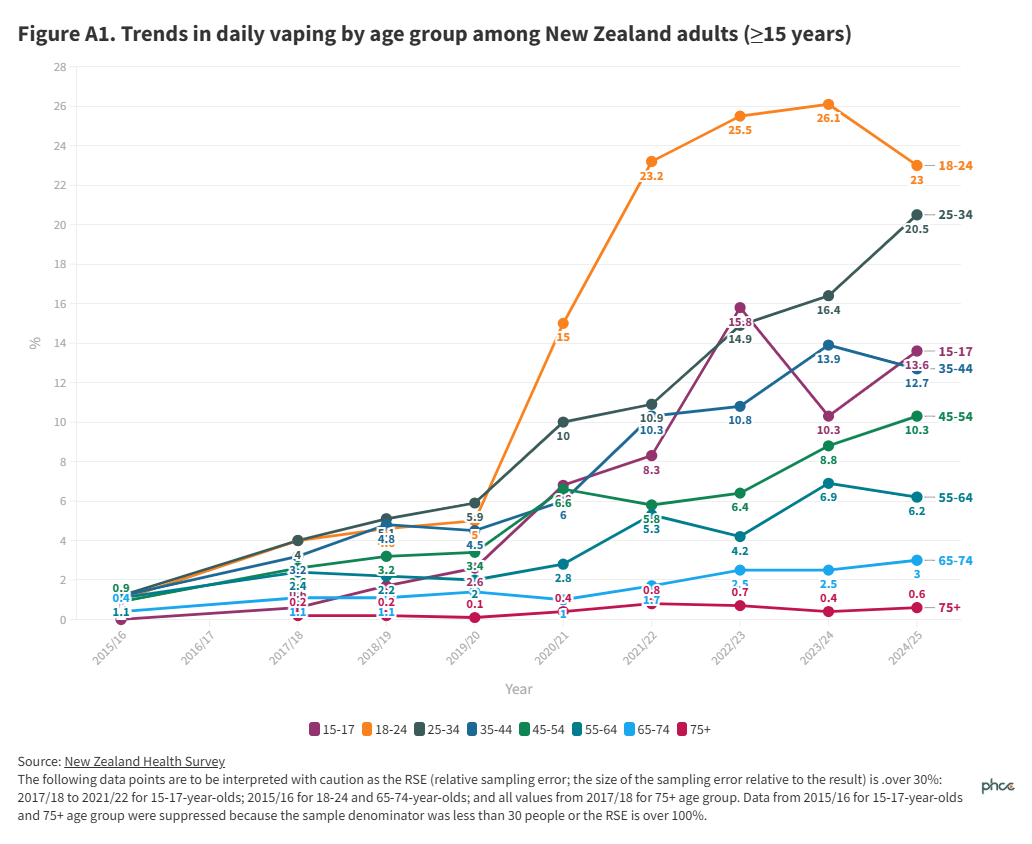
Vaping prevalence varied greatly by age and was highest among younger age groups. In 2024/25 daily vaping prevalence was 23.0% (95%CI:19.1-27.3) among 18-24-year-olds, 20.5% (95%CI: 17.8-23.4) among 25–34-year-olds and 13.6% (95%CI: 7.8-21.7) among 15-17-year-olds. The 2024/25 estimate represents 138,000 15-24-year-olds vaping daily; over a quarter of all people who vaped daily. Further details of daily and current vaping prevalence by age groups are shown in Figures A1 to A3, and Table A1 in Appendix 3.
Since 2019/20, daily vaping has increased most among 18–24-year-olds, with prevalence consistently highest in this age group since 2020/21 (Figure A1). Daily vaping among 18-24-year-olds reduced in 2024/25 compared to 2023/24 (Figure 3), but this change was not statistically significant.
Among 15–17-year-olds, daily vaping increased significantly from 2.6% (95%CI: 0.9-5.8) in 2019/20 to 10.3% (95%CI: 7.0 to 14.4) in 2023/24 and to 13.6% (95%CI: 7.8-21.7) in 2024/25 (Figure 3); however, the latter change was not statistically significant. It should be noted that, due to the small sample size of 15-17-year-olds, many estimates for this age group lack precision and should be treated with caution (summary in Figure 3 legend).
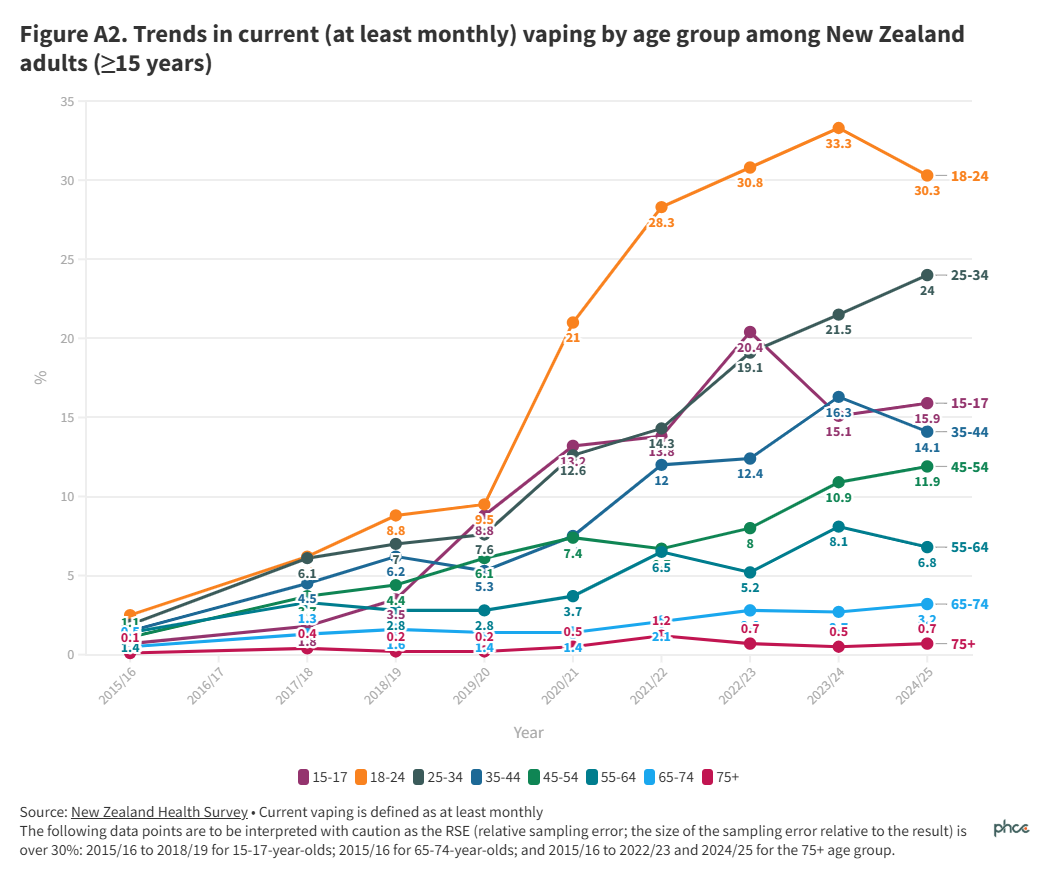
There were similar patterns and trends in current vaping by age group (Figure A2). Almost a third (30.3%, 95%CI 25.8-35.1) of 18-24-year-olds (estimated number 146,000) and one in six (15.9%, 95%CI 9.8-23.8) 15-17-year-olds (estimated number 31,000) were vaping at least monthly in 2024/25.
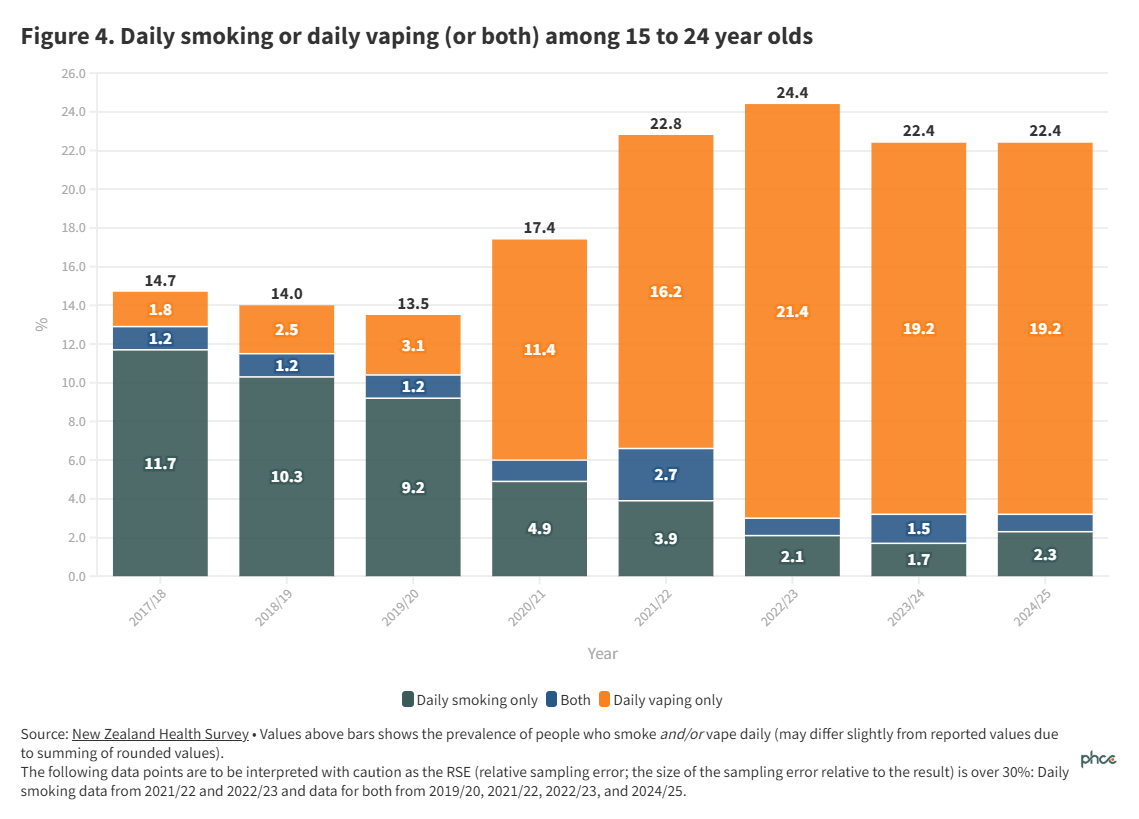
The prevalence of smoking or vaping daily (or both) among 15–24-year-olds was unchanged in 2024/25 at 22.6% (95%CI 18.9-26.6) compared to 2023/24 (Figure 4). Figure 4 shows that vaping has increased as smoking has decreased in this age group, although the absolute increase in daily vaping prevalence has been substantially greater than the decrease in daily smoking. As a result, prevalence of smoking or vaping daily (or both) increased markedly since 2017/18-2019/20 (when it was 13-15%).
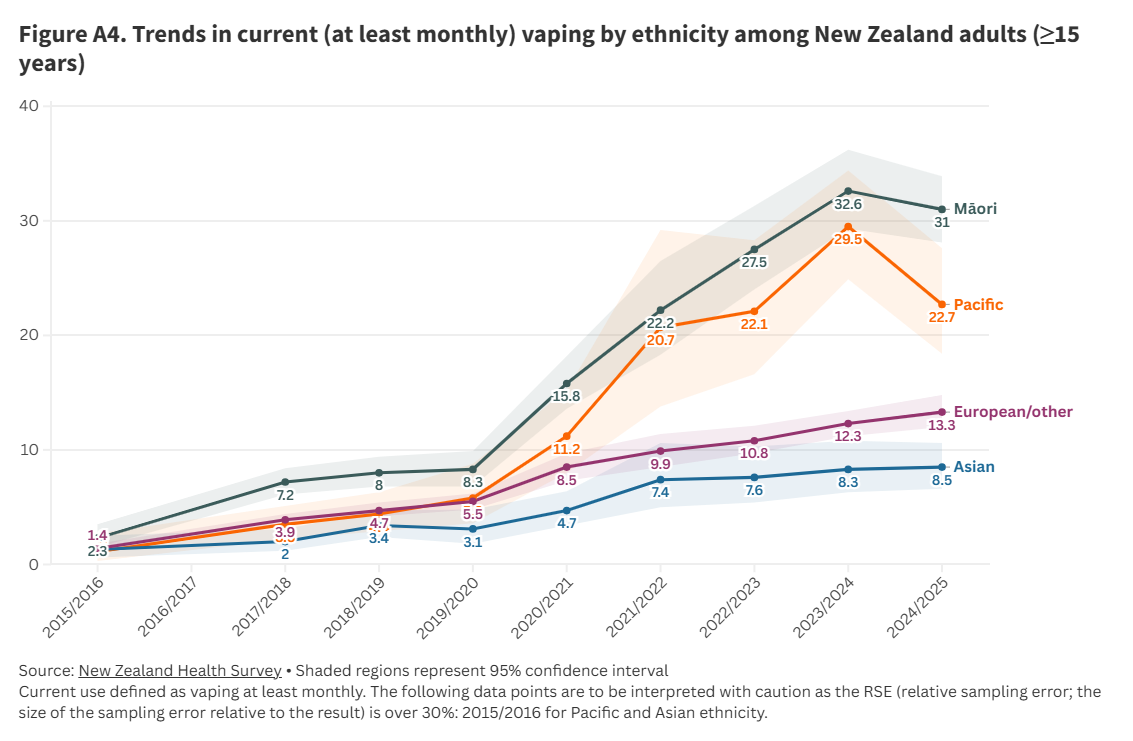
Vaping by ethnicity
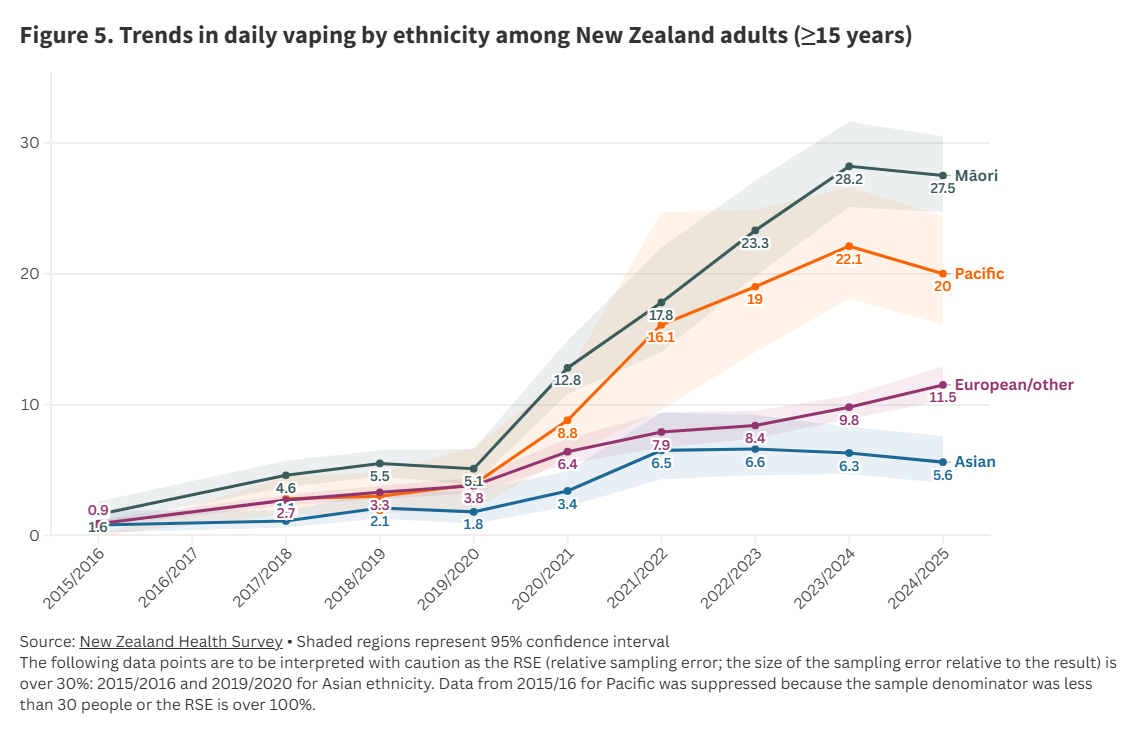
In 2024/25, daily vaping prevalence by ethnicity was highest for Māori (27.5%, 95%CI: 24.7-30.5) and for Pacific peoples (20.0%, 95%CI: 16.1-24.4), (Figure 5, Table A1). There was a statistically significant increase in daily vaping among European/Other adults from 2023/24 to 2024/25, but no statistically significant changes for other ethnicities.
When data were adjusted for age and gender, Māori were over 2.5 times more likely to vape daily than non-Māori (adjusted ratio 2.58, 95%CI: 2.26-2.95) (See Appendix 2, endnote 2) and Pacific peoples were almost one and a half times more likely to vape daily than non-Pacific (adjusted ratio 1.44, 95%CI: 1.14-1.80).
Data for current (at least monthly) vaping are presented in Figure A4.
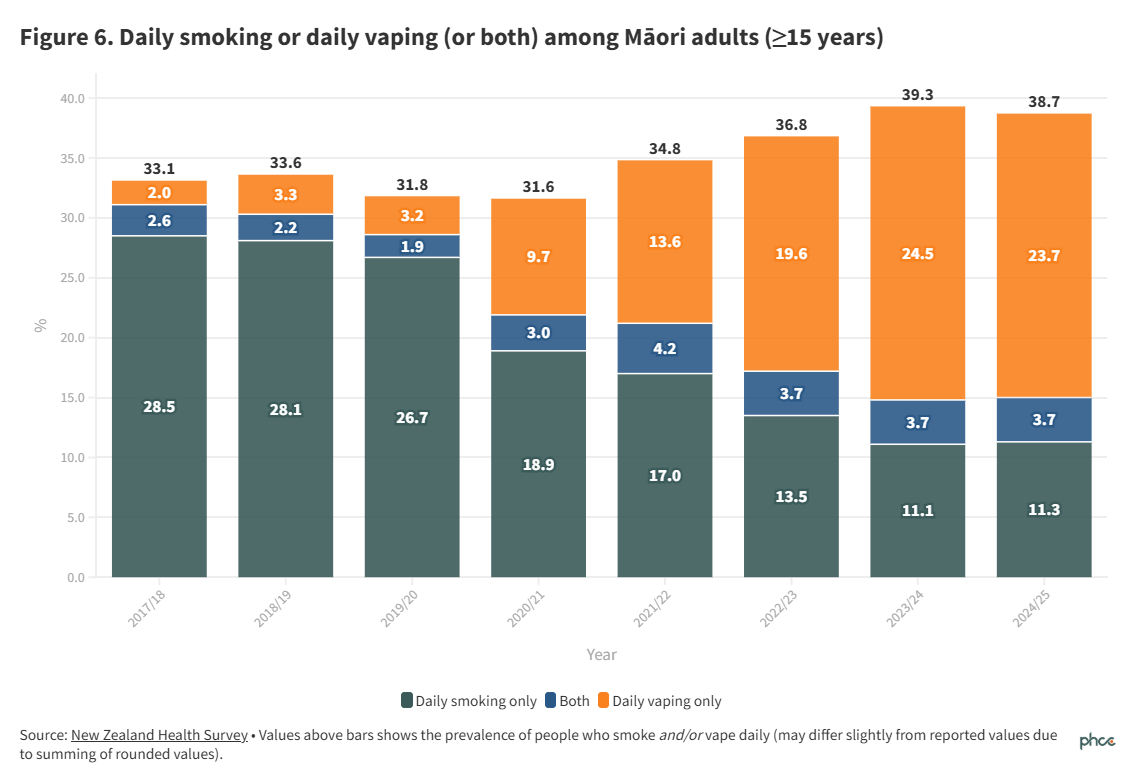
The prevalence of smoking or vaping daily (or both) was 38.8% (95%CI: 36.0-41.7) among Māori and 28.1% (95%CI: 23.8-32.7) among Pacific peoples, significantly higher than among non-Māori and non-Pacific adults respectively. Figure 6 shows that whilst daily smoking prevalence has fallen among Māori, particularly since 2021/22, prevalence of smoking or vaping daily (or both) increased after 2021/22 due to the substantial increase in daily vaping.
Vaping by neighbourhood deprivation
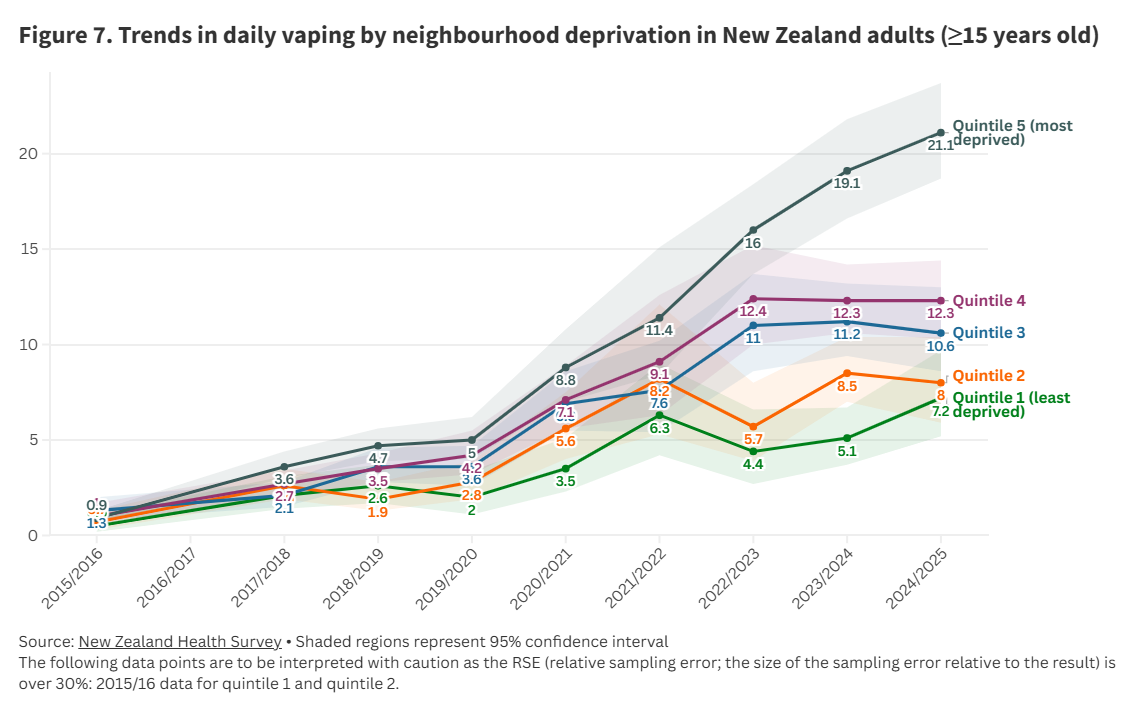
Vaping prevalence differed greatly by neighbourhood deprivation (Figure 7, Figure A5, Table A1). Daily vaping ranged from 7.2% (95%CI: 5.2-9.7) among people living in the least deprived neighbourhoods (quintile 1) (See Appendix 2. endnote 3) to 21.1% (95%CI: 18.7-23.7) among people living in the most deprived (quintile 5).
When data were adjusted (for age, gender, and ethnicity), (See Appendix 2, endnote 4) people living in quintile 5 were more than twice as likely to vape daily than people in quintile 1 (adjusted ratio 2.41, 95%CI: 1.73-3.34).
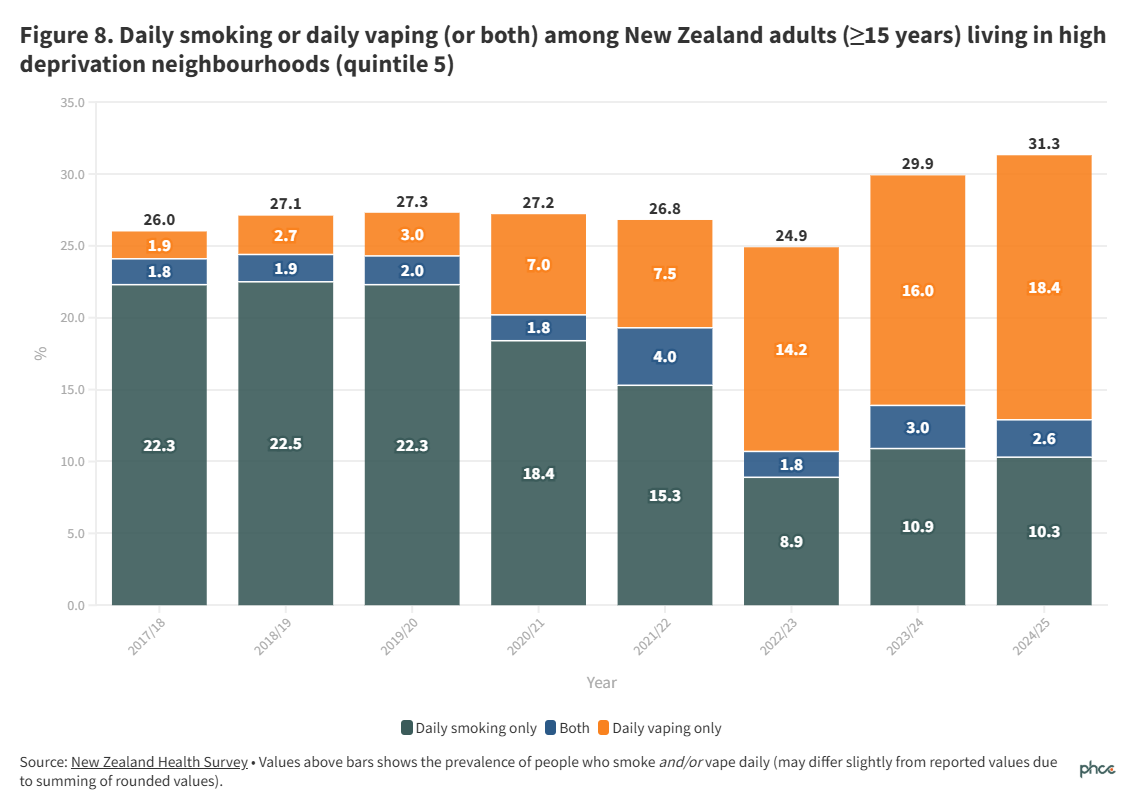
The prevalence of smoking or vaping daily (or both) was 31.4% (95%CI: 28.7-34.2) among people living in quintile 5 compared to 9.0% (95%CI: 6.9-11.5) for people living in quintile 1.
Figure 8 shows that daily smoking prevalence fell among people living in the most deprived quintile after 2019/20. However, prevalence of smoking or vaping daily (or both) increased due to large increases in daily vaping.
Conclusions
The trend of increasing vaping prevalence observed between 2019/20 and 2023/24 appears to have flattened out in 2024/25, when vaping prevalence was mostly similar to 2023/24. Previous patterns of much higher daily vaping rates among young people, Māori and Pacific peoples and people living in the most deprived neighbourhoods were largely unchanged. Further analyses are needed to examine whether, as seems highly likely, vaping is substantially higher among Māori and Pacific peoples aged 15 to 24 years than in other ethnic groups in this age group.
High rates of vaping within populations require careful interpretation. For example, high vaping rates among Māori will reflect that they are a younger population, with higher prevalences of smoking and who are more likely to live in lower decile neighbourhoods where vape retailers are concentrated.
Vaping may help to reduce smoking prevalence by providing people who smoke, and who cannot or do not wish to quit using nicotine altogether, with a less physically harmful alternative to smoking. However, full transition from smoking to vaping is required to reduce risk; dual use of both tobacco and vapes may be as harmful, or even more harmful, than smoking alone.2 Furthermore, vaping products are not harmless and remain highly addictive so uptake among adolescents and people who have never smoked poses risks to physical and mental well-being.3,4,5
Falls in daily smoking prevalence since 2019/20 have been accompanied by increases in daily vaping prevalence consistent with assertions that people are stopping smoking by switching to vaping. However, larger absolute increases in daily vaping prevalence compared to decreases in daily smoking prevalence, particularly for young people (Figure 4), have resulted in increased daily nicotine product use and suggest many young people who are vaping daily would not have smoked daily.
The findings suggest that regulatory changes introduced in 2023/24 to reduce vaping uptake among young people have not significantly reduced vaping rates, but conceivably may have slowed the increase in vaping uptake. Regulations introduced in June 2025 were implemented after almost all of the 2024/25 survey data collection had been completed, so their impact cannot be assessed using these data. There is somewhat contrasting data from the Year 10 Snapshot survey showing daily vaping prevalence among 14-15 year olds has declined since around 2023.
The very high prevalence of vaping among young people and priority groups indicates the need for thorough and timely evaluation of recent regulatory changes and the enforcement of these. Unless these reduce vaping prevalence substantially and equitably, further measures to protect young people from becoming addicted to vaping, while maintaining reasonable access for people who smoke and wish to switch to vaping, will be required. Such actions could include further flavour restrictions, introduction of excise taxes to reduce the affordability of low cost vapes, and interventions to reduce the accessibility of vapes, such as ending sales in non-specialist retailers like dairies, service stations and supermarkets.
What this Briefing adds
- The prevalence of daily vaping in 2024/25 was 11.7%, representing an estimated 509,000 people, including 138,000 aged 15-24 years.
- Vaping is most prevalent among 18-24-year-olds, Māori and Pacific peoples, and people living in the most deprived neighbourhoods.
Implications for policy and practice
- Unless recently-introduced measures reduce high rates of vaping among adolescents and young people, additional strengthening of the regulatory framework for vaping products is likely to be required to protect young people from becoming addicted to vaping.
Acknowledgements
The authors acknowledge the New Zealand Health Survey team at the Ministry of Health who carry out and report the NZHS. The 2024/25 Annual Update of Key Results is available online at: https://www.health.govt.nz/publications/annual-update-of-key-results-202425-new-zealand-health-survey
Authors details
Prof Richard Edwards, ASPIRE Aotearoa Research Centre, and Head of Public Health, College of Medicine & Public Health | Flinders University
Dr Janine Nip, ASPIRE Aotearoa Research Centre, and Department of Public Health, ŌtākouWhakaihu Waka | University of Otago
Prof Janet Hoek, Co-Director of ASPIRE Aotearoa Research Centre, and Department of Public Health, Ōtākou Whakaihu Waka | University of Otago
Assoc Prof Andrew Waa, Co-Director of ASPIRE Aotearoa Research Centre, and Department of Public Health, Ōtākou Whakaihu Waka | University of Otago
Dr Jude Ball, Co-Director of ASPIRE Aotearoa Research Centre, and Department of Public Health, Ōtākou Whakaihu Waka | University of Otago
2023 (September)
- New specialist vaping retailers must be at least 300 metres from schools and marae.
2023 (December)
- New maximum nicotine concentration.
- Single-use devices required to have removable batteries and a child safety mechanism.
2024 (March)
- Updated maximum nicotine concentrations, restrictions on flavour descriptors, and a ban on cartoons and images of toys on packaging.
2024 (October)
- All vaping devices required to have removable batteries and a child safety mechanism.
2024 (December)
- Increased penalties for sales to minors.
- New specialist vape retailers cannot open within 100 metres of an early childhood education centre.
2025 (June)
- Vaping devices, products, and packaging must not be visible in general retailers
- Vaping devices, products, and packaging must not be visible from outside store for specialist vape retailers.
- Online store product display ban.
- Sale of disposable vapes prohibited.
- Vape discounts, promotion and product giveaways prohibited.
2025 (September)
- Requirement for removable batteries for all vaping products revoked.
Appendix 2
New Zealand Health Survey: Methodological details and endnotes
The NZHS is an annual nationally representative population survey that has run since 2011/12. In 2024/25, the adult survey included data collected from 9,253 New Zealanders aged 15 years and older from 9 July 2024 to 20 July 2025.
Data include 95% confidence intervals (95%CI), which indicate the uncertainty in an estimate.
Endnote 1: Further detail on confidence intervals is in the NZHS methodology report). A summary of the 2024/25 data is in Appendix 3 (Table A1).
Endnote 2: Adjusted ratios with adjustment variables are as presented on the Ministry of Health website. An adjusted ratio of above 1 indicates an outcome is more likely in a group of interest, for example an adjusted ratio of 2 means an outcome is 2 times more likely in the group of interest compared with the reference group.
Endnote 3: In the NZHS, neighbourhood deprivation refers to the New Zealand Index of Deprivation 2018 (NZDep2018), which measures the level of socioeconomic deprivation for each neighbourhood (Statistical Area 1) according to a combination of the following 2018 Census variables: household income, benefit receipt, household crowding, home ownership, employment status, qualifications, single parent families, living in home with dampness/mould and access to the internet. Quintile 1 represents areas with the lowest level of deprivation and quintile 5 represents the highest level of deprivation. Further detail is available in the NZHS methodology report.
Endnote 4: Although these estimates are technically “adjusted” for ethnic differences, we do not interpret this adjustment as capturing a causal effect of ethnicity. Rather, it reflects the likely confounding influence of unmeasured variables that vary by ethnicity and are associated with key outcomes.
Appendix 3 Additional results
Table A1. Data for current and daily vaping prevalence with confidence intervals in 2024/25 New Zealand Health Survey
| | Current vaping (at least monthly) | Daily vaping | Daily vaping or daily smoking (or both) |
| | % | (95% CI) | % | (95% CI) | % | (95% CI) |
| Total | 13.8 | ( 12.8 - 15.0 ) | 11.7 | (10.7 – 12.8 ) | 17.1 | ( 16.1 - 18.3 ) |
Age group
(years) | | | | | | |
| 15-17 | 15.9 | ( 9.8 - 23.8 ) | 13.6 | ( 7.8 – 21.7 ) | 13.9 | ( 8.0 - 21.9 ) |
| 18-24 | 30.3 | ( 25.8 - 35.1 ) | 23.0 | ( 19.1 – 27.3) | 26.1 | ( 22.0 - 30.6 ) |
| 25-34 | 24.0 | ( 21.2 - 27.0 ) | 20.5 | ( 17.8 - 23.4 ) | 25.5 | ( 22.6 - 28.7 ) |
| 35-44 | 14.1 | ( 11.8 - 16.6 ) | 12.7 | ( 10.6 - 15.2) | 18.2 | ( 15.6 - 21.1 ) |
| 45-54 | 11.9 | ( 9.7 - 14.4 ) | 10.3 | ( 8.1 – 12.7 ) | 17.4 | ( 14.9 - 20.1 ) |
| 55-64 | 6.8 | ( 5.2 - 8.7 ) | 6.2 | ( 4.6 - 8.1 ) | 15.0 | ( 12.9 - 17.2 ) |
| 65-74 | 3.2 | ( 2.3 - 4.4 ) | 3.0 | ( 2.1 - 4.2 ) | 8.5 | ( 6.8 - 10.3 ) |
| 75+ | 0.7* | ( 0.3 - 1.3 ) | 0.6* | ( 0.2 - 1.2 ) | 3.7 | ( 2.4 - 5.3 ) |
| Ethnic group | | | | | | |
| Māori | 31.0 | ( 28.1 - 33.9 ) | 27.5 | ( 24.7 - 30.5 ) | 38.8 | ( 36.0 - 41.7 ) |
| Pacific | 22.7 | ( 18.4 - 27.6 ) | 20.0 | ( 16.1 – 24.4 ) | 28.1 | ( 23.8 - 32.7 ) |
| Asian | 8.5 | ( 6.6 - 10.6 ) | 5.6 | ( 4.0 - 7.6 ) | 8.9 | ( 7.1 - 11.0 ) |
| European/Other | 13.3 | ( 12.0 - 14.8 ) | 11.5 | ( 10.3 - 12.9 ) | 16.1 | ( 14.7 - 17.6 ) |
Neighbourhood
deprivation | | | | | | |
Quintile 1
(least deprived) | 8.1 | ( 6.0 - 10.6 ) | 7.2 | ( 5.2 - 9.7 ) | 9.0 | ( 6.9 - 11.5 ) |
| Quintile 2 | 9.9 | ( 7.5 - 12.8 ) | 8.0 | ( 5.9 – 10.4 ) | 12.2 | ( 10.2 - 14.6 ) |
| Quintile 3 | 12.5 | ( 10.5 - 14.8 ) | 10.6 | ( 8.6 - 13.0 ) | 15.2 | ( 12.9 - 17.8 ) |
| Quintile 4 | 14.9 | ( 12.6 - 17.5 ) | 12.3 | ( 10.3 - 14.4 ) | 18.6 | ( 16.5 - 20.9 ) |
Quintile 5
(most deprived) | 24.3 | ( 21.9 - 26.7 ) | 21.1 | ( 18.7 – 23.7 ) | 31.4 | ( 28.7 - 34.2 ) |
95% CI: 95% confidence interval.
*data recommended to be interpreted with caution as the RSE (relative sampling error; the size of the sampling error relative to the result) is over 30%
Daily smoking is defined as: smoking every day and smoked more than 100 cigarettes in whole life