Summary
New Zealand Health Survey (NZHS) data for 2023/2024 have been released. Daily vaping prevalence among adults aged ≥15 years increased from 3.5% in 2019/20 to 11.1% in 2023/24.
Vaping prevalence was particularly high among younger age groups, Māori and Pacific peoples, and people living in neighbourhoods with higher levels of deprivation.
The findings call for detailed ongoing monitoring and research to assess whether the current regulatory settings protect people who do not smoke (particularly young people) from highly addictive products and also support people who smoke to switch to a nicotine source that poses fewer physical harms.
Vapes (also known as electronic cigarettes) may help to reduce smoking prevalence by offering people who smoke a less physically harmful alternative to smoking. However, vaping products are not harmless and can be highly addictive.
Recent rapid increases in vaping among young people have created great concern among parents, communities and schools, and health workers. Successive governments have proposed measures to regulate vaping products, but debate continues over whether regulation is overly restrictive or too permissive.
This Briefing summarises key updates on vaping prevalence from the 2023/24 New Zealand Health Survey (NZHS). An accompanying Briefing provides information on smoking prevalence.1
Key findings
Population trends
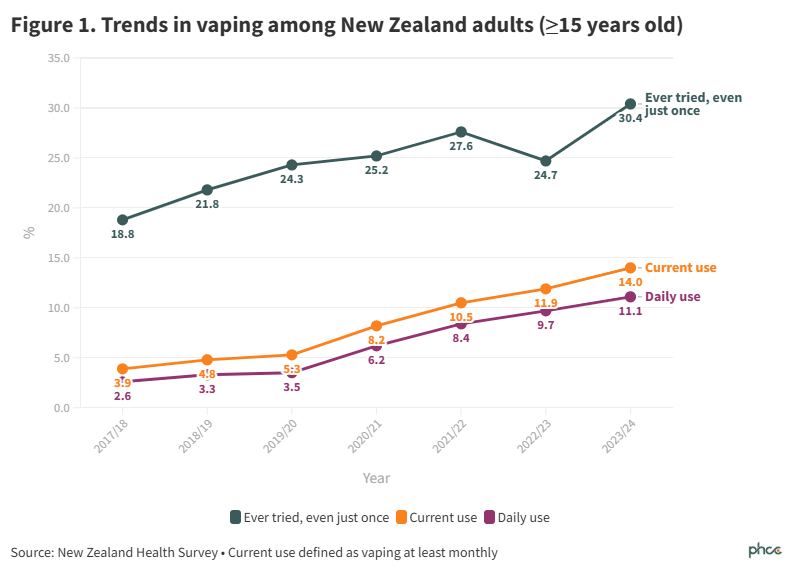
Adult daily vaping prevalence increased steadily from 3.5% (95%CI: 3.0-4.1) in 2019/20 to 11.1% (95% confidence interval [CI]: 10.3-11.9) in 2023/24. This represents an estimated 480,000 people vaping daily in 2023/24 (Figure 1, Appendix Table A1). The increase in prevalence from 9.7% (95%CI: 8.9-11.8) in 2022/23 was not statistically significant.
Most people who vape currently (at least monthly) are vaping daily (79% in 2023/24).
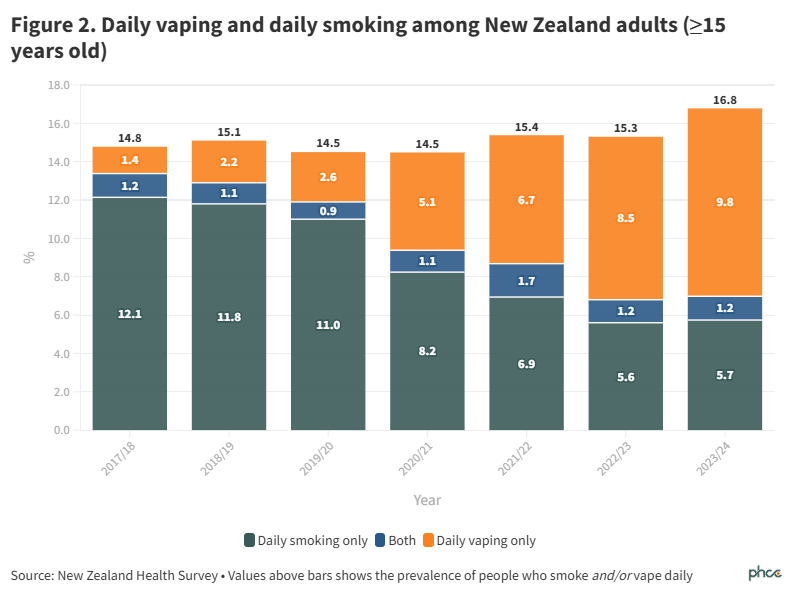
For the first time, the NZHS data explorer provided data on sole and dual use of vapes and cigarettes (Figure 2). Increases in vaping have been greater than decreases in smoking, which has led to a small but statistically significant increase in the prevalence of people smoking daily and/or vaping daily between 2018/19 and 2023/24 (from 15.1% (95%CI: 14.3-16.0) to 16.8% (95%CI: 15.8-17.8), p<0.01). This change was likely driven by substantial increases in vaping among 15–24-year-olds, as shown in Figure 3.
Vaping by age group
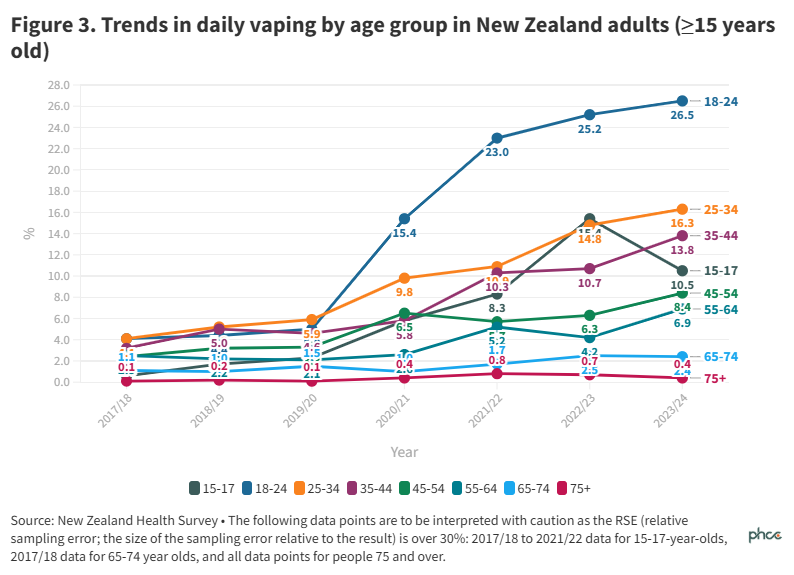
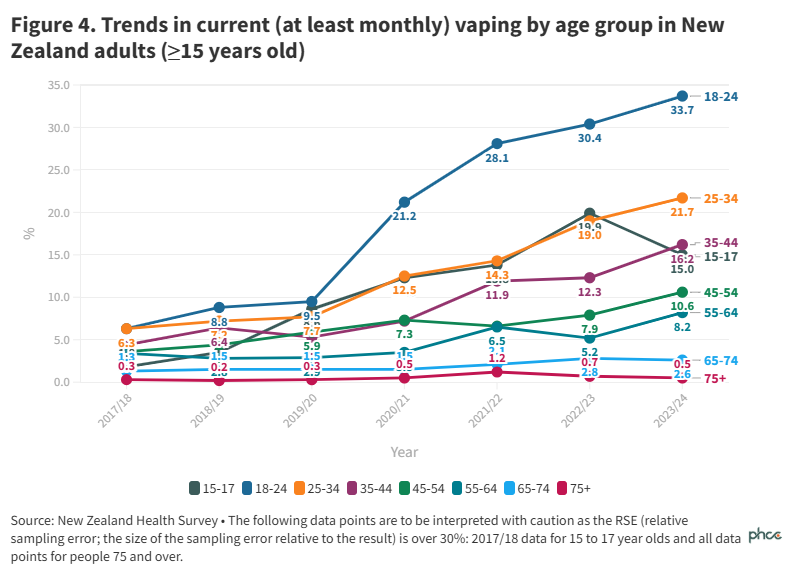
Since 2020/21, 18–24-year-olds consistently had the highest prevalences of vaping (Figures 3 and 4, Table A1). Daily vaping in this age group increased to 26.5% (95%CI: 22.2-31.1) in 2023/24, representing an estimated 119,000 people and around a quarter of all people who vape daily.
The next highest prevalence was 16.3% (95%CI: 14.3-18.5) among 25–34-year-olds, representing an estimated 126,000 people.
Among 15–17-year-olds, daily vaping prevalence increased to a peak of 15.4% (95%CI: 10.3-21.9) in 2022/23 and declined to 10.5% (95%CI: 7.1-14.9) in 2023/24, however, the decline was not statistically significant.
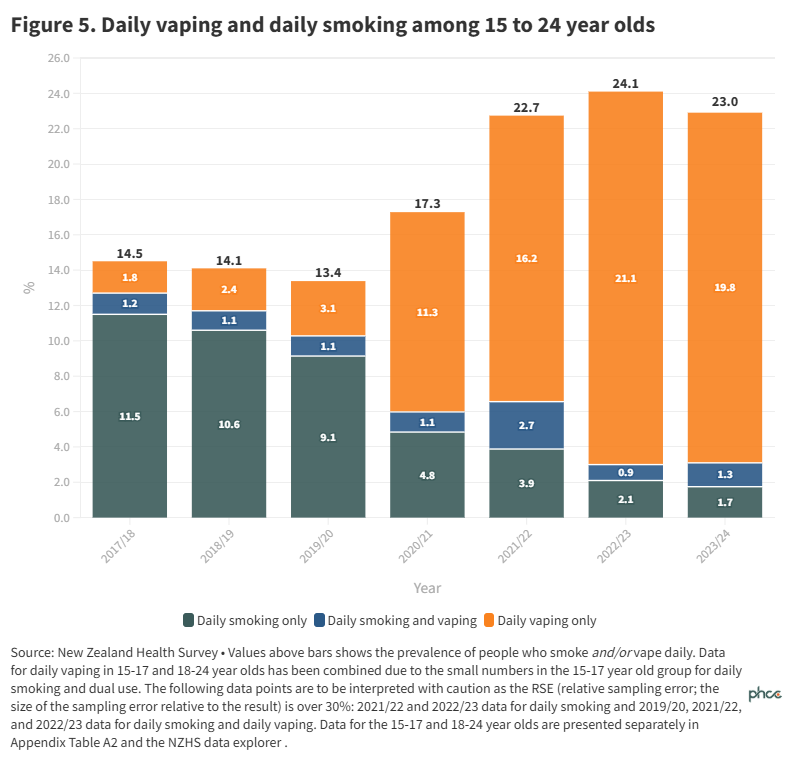
The prevalence of smoking and/or vaping among 15–24-year-olds was 13-15% from 2017/18 to 2019/20 (Figure 5). It then increased to 22-24% from 2021/22 (Figure 5). The increase was due to a large increase in daily vaping prevalence, much greater in absolute terms than the decline in smoking prevalence. In contrast, there was no statistically significant change in prevalence of daily and/or daily vaping for other age groups between 2018/19 and 2023/24 (Table A2).
Vaping by ethnicity
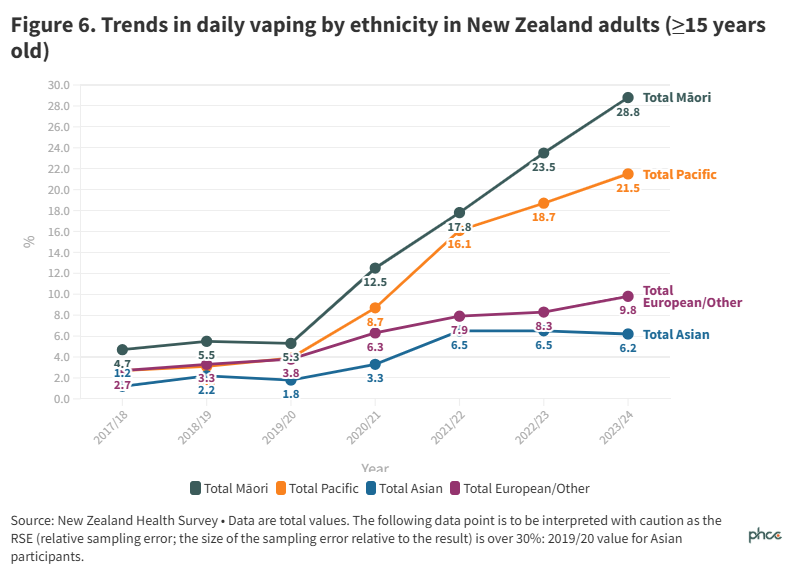
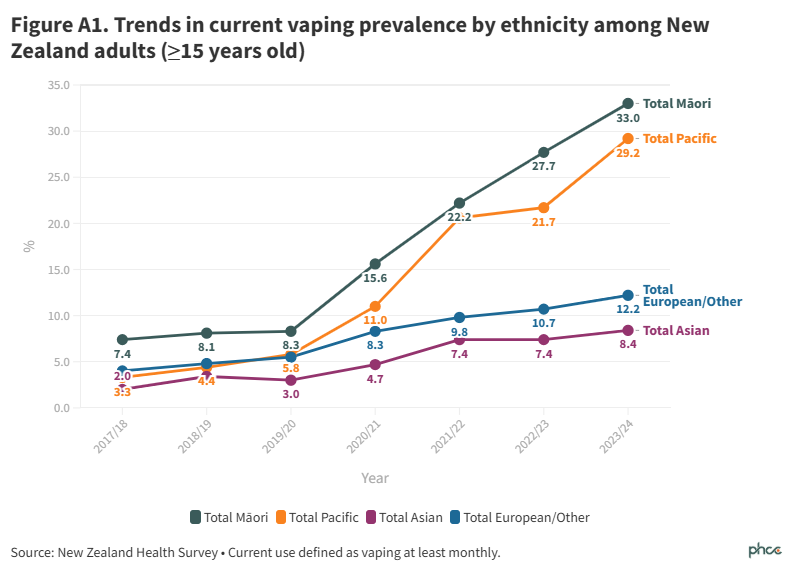
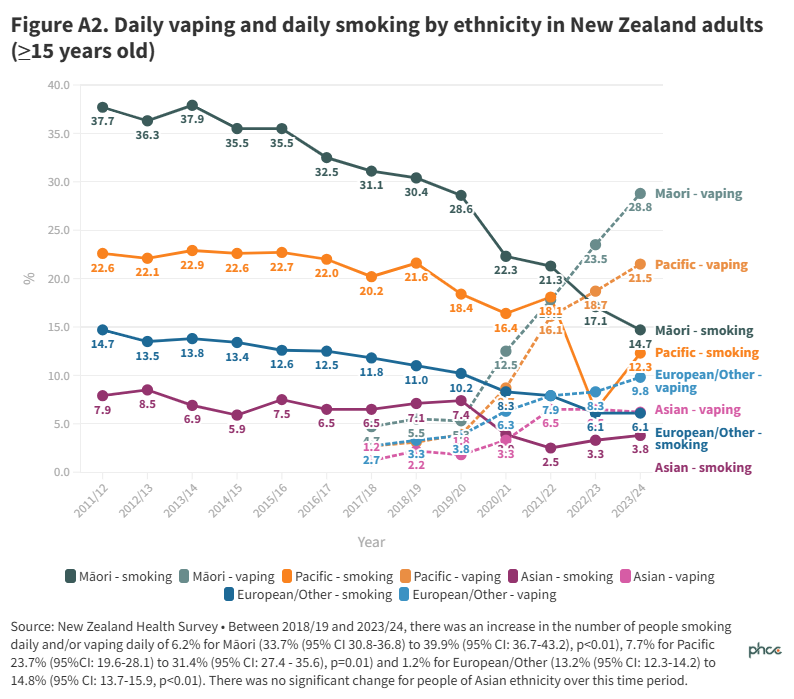
In 2023/24, daily vaping prevalences reached 28.8% (95%CI: 25.6-32.1) for Māori and 21.5% (95%CI: 17.5-25.9) for Pacific peoples (Figure 6, Table A1). Data for current (at least monthly) vaping are presented in Figure A1).
When data were adjusted (for age and gender), Māori were three times more likely to vape than non- Māori (adjusted ratio 2.99, 95% CI: 2.49-3.60) and Pacific peoples were over one and a half times more likely to vape than non-Pacific (adjusted ratio 1.65, 95%CI: 1.34-2.01).
Between 2011/12 and 2023/24, the overall pattern of smoking prevalence has been higher for Māori and Pacific peoples, compared to non-Māori/non-Pacific (Figure A2). The absolute increase in vaping prevalence among Māori, Pacific peoples, and European/Other has been greater than the absolute reduction in smoking prevalence over this period (Figure A2).
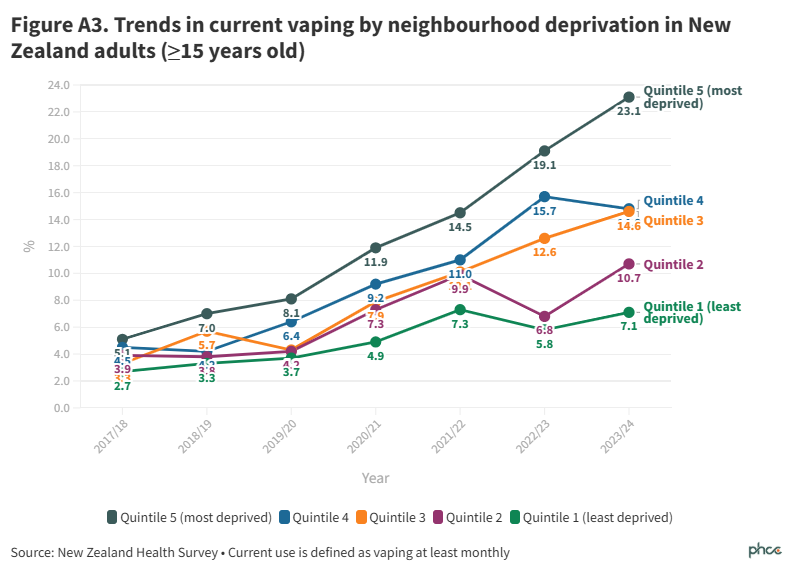
Vaping by neighbourhood deprivation
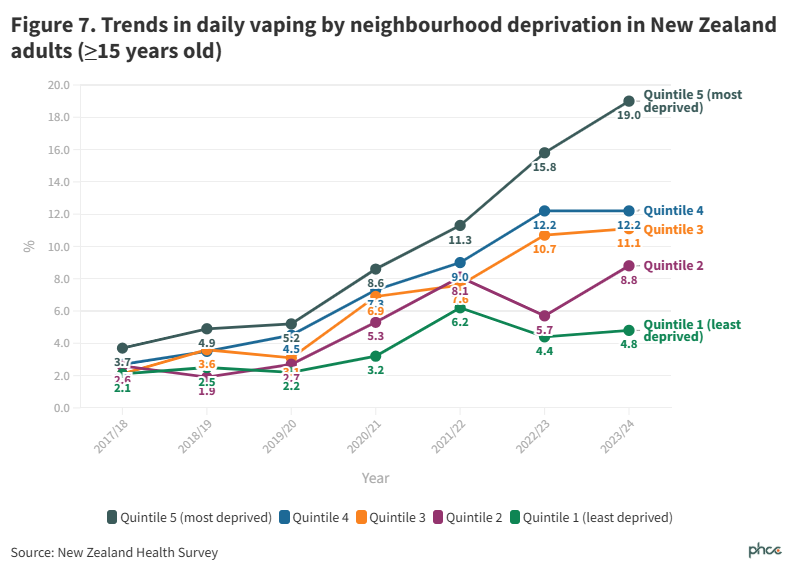
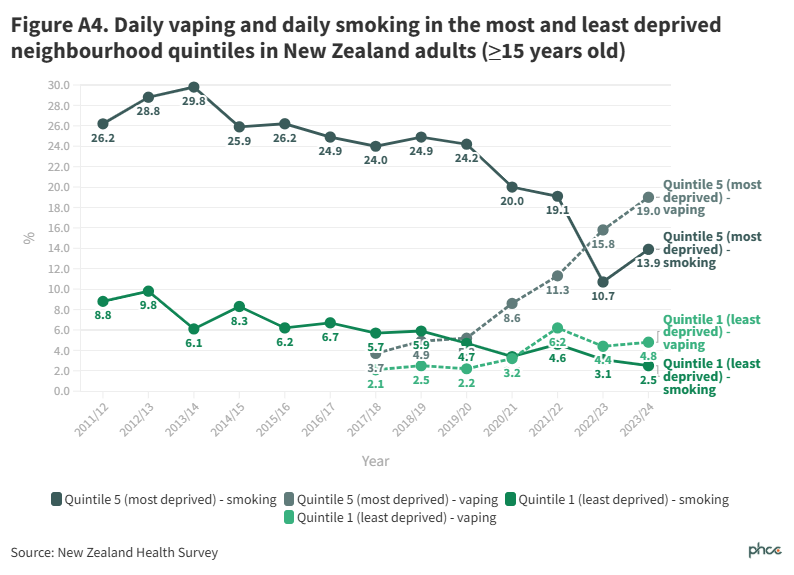
In 2023/24, vaping prevalence differed greatly by neighbourhood deprivationNote (Figure 7, Figure A3); daily vaping ranged from 4.8% (95%CI: 3.4-6.6) in quintile 1 (least deprived) to 19.0% (95%CI: 16.4-21.8) in quintile 5 (most deprived).
When data were adjusted (for age, gender, and ethnicity), people living in quintile 5 were more than twice as likely to vape daily than people in quintile 1 (adjusted ratio 2.27, 95%CI: 1.67-3.09).
To view recent vaping trends in the context of smoking trends for people living in the areas of highest and lowest neighbourhood deprivation, see Figure A4.
Conclusions
Adult daily vaping prevalence has continued to increase, reaching 11.1% in 2023/24, which represents an estimated 480,000 people. The declines in smoking prevalence over the same period could suggest some people who smoked now use vapes as a substitute nicotine product.
Patterns for 15–24-year-olds differ to those for older adults. The prevalence of daily vaping and/or daily smoking in this age group almost doubled between 2019/20 and 2023/24 (13.4% to 23.0%). This suggests that much of the increase is due to people who have never smoked taking up vaping, rather than people using vaping as a substitute for smoking.
Vaping is more prevalent among Māori and Pacific peoples, and people living in more deprived neighbourhoods. It is important to note differences in vaping prevalence reflect inequities experienced by people who identify as Māori and Pacific, as well as structural factors, such as the concentration of vape retailers in more deprived neighbourhoods.
The findings highlight the importance of continuing to evaluate and, where necessary, strengthen the regulatory framework for vaping products so people who do not smoke, particularly young people, are protected from becoming addicted to vaping, while people who smoke and wish to switch to vaping still have reasonable access to these products.2
What this Briefing adds
- The prevalence of daily vaping in 2023/24 was 11.1%, representing an estimated 480,000 people.
- Vaping is most prevalent among 18-24 year olds, Māori and Pacific peoples, and people living in the most deprived neighbourhoods.
Implications for policy and practice
- Further measures to strengthen vaping regulation will likely be required to prevent people who do not smoke from taking up vaping, while allowing reasonable access to these products for people who smoke.
Authors details
Dr Janine Nip, Prof Richard Edwards, Prof Janet Hoek, Assoc Prof Andrew Waa, Dr Jude Ball, Dr Michaela Pettie
All authors are members of ASPIRE Aotearoa and the Department of Public Health, Ōtākou Whakaihu Waka | University of Otago, Wellington
Footnote: The NZHS uses the New Zealand Index of Deprivation 2018 (NZDep2018), which measures the level of socioeconomic deprivation according the following 2018 Census variables: household income, benefit receipt, household crowding, home ownership, employment status, qualifications, single parent families, living in home with dampness/mould, and access to the internet.
Appendix
About the New Zealand Health Survey
The NZHS is an annual, nationally representative population survey. It aims to sample around 14,000 adults aged 15 years and over every year. Detailed methods of the survey and access to data presented in this article are available on the Ministry of Health website.
Table A1. Data for daily vaping prevalence with confidence intervals
| | 2021/22 | 2022/23 | 2023/24 |
| | % | (95% CI) | % | (95% CI) | % | (95% CI) |
| Total | 8.4 | ( 7.2 - 9.8 ) | 9.7 | ( 8.8 - 10.7 ) | 11.1 | ( 10.3 - 11.9 ) |
| Age group (years) | | | | | | |
| 15-17 | 8.3 e | ( 3.8 - 15.5 ) | 15.4 | ( 10.3 - 21.9 ) | 10.5 | ( 7.1 - 14.9 ) |
| 18-24 | 23.0 | ( 16.3 - 31.0 ) | 25.2 | ( 19.3 - 31.9 ) | 26.5 | ( 22.2 - 31.1 ) |
| 15-24 | 18.8 | ( 13.7 - 24.9 ) | 22.1 | ( 17.9 - 26.7 ) | 21.3 | ( 18.0 - 24.8 ) |
| 25-34 | 10.9 | ( 8.1 - 14.3 ) | 14.8 | ( 12.5 - 17.4 ) | 16.3 | ( 14.3 - 18.5 ) |
| 35-44 | 10.3 | ( 7.9 - 13.1 ) | 10.7 | ( 8.3 - 13.5 ) | 13.8 | ( 11.9 - 15.9 ) |
| 45-54 | 5.7 | ( 3.8 - 8.3 ) | 6.3 | ( 4.6 - 8.3 ) | 8.4 | ( 6.9 - 10.1 ) |
| 55-64 | 5.2 | ( 3.6 - 7.3 ) | 4.2 | ( 3.1 - 5.5 ) | 6.9 | ( 5.2 - 8.9 ) |
| 65-74 | 1.7 | ( 1.0 - 2.7 ) | 2.5 | ( 1.4 - 4.1 ) | 2.4 | ( 1.6 - 3.5 ) |
| 75+ | 0.8 e | ( 0.2 - 2.4 ) | 0.7 e | ( 0.2 - 1.8 ) | 0.4 e | ( 0.2 - 0.8 ) |
| Ethnic group (total) | | | | | | |
| Māori | 17.8 | ( 14.1 - 22.0 ) | 23.5 | ( 19.8 - 27.4 ) | 28.8 | ( 25.6 - 32.1 ) |
| Pacific | 16.1 | ( 9.6 - 24.6 ) | 18.7 | ( 13.8 - 24.5 ) | 21.5 | ( 17.5 - 25.9 ) |
| Asian | 6.5 | ( 4.3 - 9.3 ) | 6.5 | ( 4.6 - 8.9 ) | 6.2 | ( 4.5 - 8.3 ) |
| European/Other | 7.9 | ( 6.6 - 9.3 ) | 8.3 | ( 7.3 - 9.4 ) | 9.8 | ( 8.8 - 10.7 ) |
| Neighbourhood deprivation | | | | | | |
| Quintile 1 (least deprived) | 6.2 | ( 4.1 - 8.9 ) | 4.4 | ( 2.7 - 6.7 ) | 4.8 | ( 3.4 - 6.6 ) |
| Quintile 2 | 8.1 | ( 5.2 - 12.0 ) | 5.7 | ( 3.8 - 8.2 ) | 8.8 | ( 7.1 - 10.7 ) |
| Quintile 3 | 7.6 | ( 5.5 - 10.2 ) | 10.7 | ( 8.4 - 13.4 ) | 11.1 | ( 9.1 - 13.2 ) |
| Quintile 4 | 9.0 | ( 6.3 - 12.5 ) | 12.2 | ( 9.8 - 14.9 ) | 12.2 | ( 10.5 - 14.2 ) |
| Quintile 5 (most deprived) | 11.3 | ( 8.3 - 15.0 ) | 15.8 | ( 13.6 - 18.3 ) | 19.0 | ( 16.4 - 21.8 ) |
Table A2. Prevalence daily vaping and/or daily smoking by age group across years. The rightmost column displays p values for the difference between 2018/19 and 2023/24.
| | Percentage (95% confidence interval) | p |
| Age group (years) | 2017/18 | 2018/19 | 2019/20 | 2020/21 | 2021/22 | 2022/23 | 2023/24 | |
| 15-17 | 3.6
(2.1 - 5.6) | 3.9
(2.4 - 6.1) | 5.1
(2.8 - 8.4) | 6.6
(3.3 - 11.5) | 9.0e
(4.3 - 16.1) |
15.9
(10.6 - 22.4) | 10.7
(7.3 - 15.1) | <0.01 |
| 18-24 | 19.2
(16.8 - 21.8) | 18.9
(16.1 - 22.0) | 16.7
(13.7 - 20.1) | 22.0
(18.4 - 25.9) | 28.2
(21.6 - 35.5) | 28.1
(22.2 - 34.5) | 28.9
(24.5 - 33.7) | <0.01 |
| 15-24 combined | 14.5
(12.7 - 16.4) | 14.1
(12.1 - 16.3) | 13.4
(11.2 - 15.9) | 17.3
(14.5 - 20.4) | 22.7
(17.7 - 28.2) | 24.1
(19.9 - 28.8) | 23.0
(19.7 - 26.6) | <0.01 |
| | | | | | | | | |
| 25-34 | 21.6
(19.3 - 24.2) | 19.9
(17.7 - 22.2) | 21.7
(19.2 - 24.3) | 19.6
(17.2 - 22.3) | 18.3
(15.0 - 22.0) | 20.5
(17.6 - 23.7) | 22.0
(19.9 - 24.3) | 0.12 |
| 35-44 | 16.9
(15.2 - 18.8) | 21.8
(19.3 - 24.4) | 16.3
(14.1 - 18.8) | 15.0
(12.8 - 17.5) | 17.6
(14.2 - 21.5) | 16.7
(14.1 - 19.7) | 19.0
(16.7 - 21.4) | 0.09 |
| 45-54 | 15.8
(14.0 - 17.8) | 16.4
(14.4 - 18.6) | 16.9
(14.9 - 19.0) | 17.2
(14.9 - 19.7) | 14.8
(11.7 - 18.4) | 13.8
(11.4 - 16.5) | 18.1
(15.6 - 20.8) | 0.31 |
| 55-64 | 15.3
(13.4 - 17.3) | 13.1
(11.7 - 14.6) | 13.2
(11.1 - 15.6) | 14.0
(12.1 - 16.1) | 14.7
(12.0 - 17.9) | 12.9
(10.5 - 15.5) | 15.0
(12.6 - 17.6) | 0.14 |
| 65-74 | 7.4
(6.1 - 8.9) | 8.1
(6.8 - 9.6) | 7.4
(5.9 - 9.2) | 6.9
(5.4 - 8.5) | 8.2
(6.1 - 10.7) | 8.1
(6.1 - 10.4) | 8.2
(6.4 - 10.3) | 0.96 |
| 75+ | 2.2
(1.5 - 3.2) | 3.9
(2.9 - 5.2) | 3.9
(2.8 - 5.4) | 2.6
(1.8 - 3.8) | 3.6
(2.2 - 5.5) | 3.0
(1.9 - 4.4) | 3.4
(2.5 - 4.5) | 0.58 |
Note: ‘e’ means interpret with caution as the RSE (relative sampling error; the size of the sampling error relative to the result) is over 30%. Values are unadjusted prevalence percentages.